

A Multicenter Analysis of 3 Decades of Hip Arthroscopy: Evolving Techniques and Growing Patient Volumes From 1988 to 2022
- PMID: 39399769
- PMCID: PMC11467985
- DOI: 10.1177/23259671241277793
A Multicenter Analysis of 3 Decades of Hip Arthroscopy: Evolving Techniques and Growing Patient Volumes From 1988 to 2022
Abstract
Background: The number of hip arthroscopies performed in the United States has grown significantly over the past several decades, with evolving indications and emerging techniques.
Purposes: To (1) examine the evolution of hip arthroscopy at 3 tertiary referral centers between 1988 and 2022 and (2) quantify trends in patient demographics and procedures performed.
Study design: Case series; Level of evidence, 4.
Methods: A retrospective analysis was performed of all patients undergoing hip arthroscopy at 3 academic centers between 1988 and 2022. Demographic data were collected using standardized forms and operative notes, and intraoperative images were manually reviewed for each patient to determine the specific procedures performed at the time of the hip arthroscopy. Surgical procedures were plotted over time to evaluate trends. Patients were divided into 3 time periods for comparison: early hip arthroscopy from 1988 to 2008, 2009 (the time of the first labral repair in our cohort) to 2015, and 2016 to 2022.
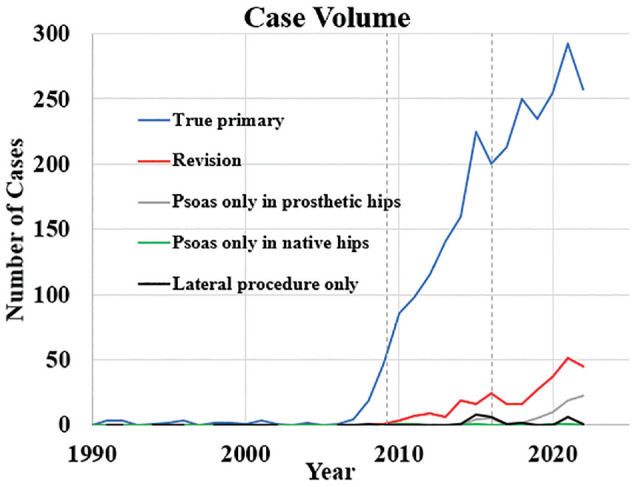
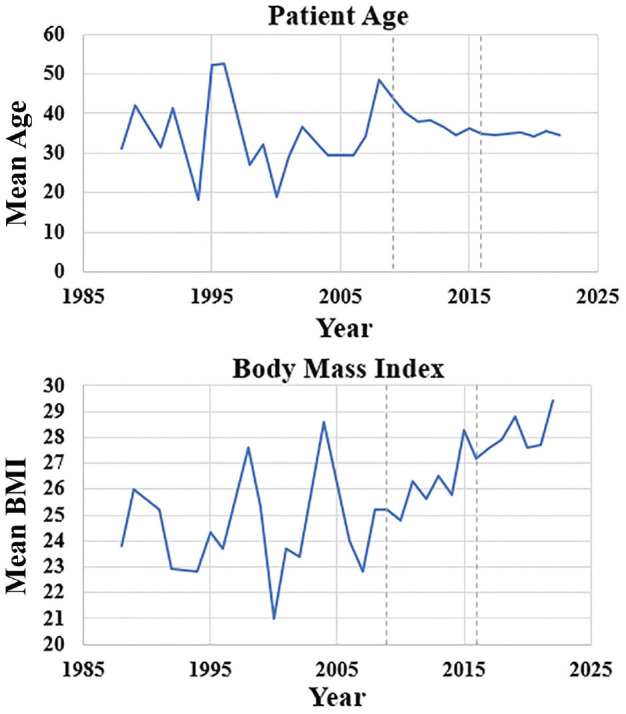
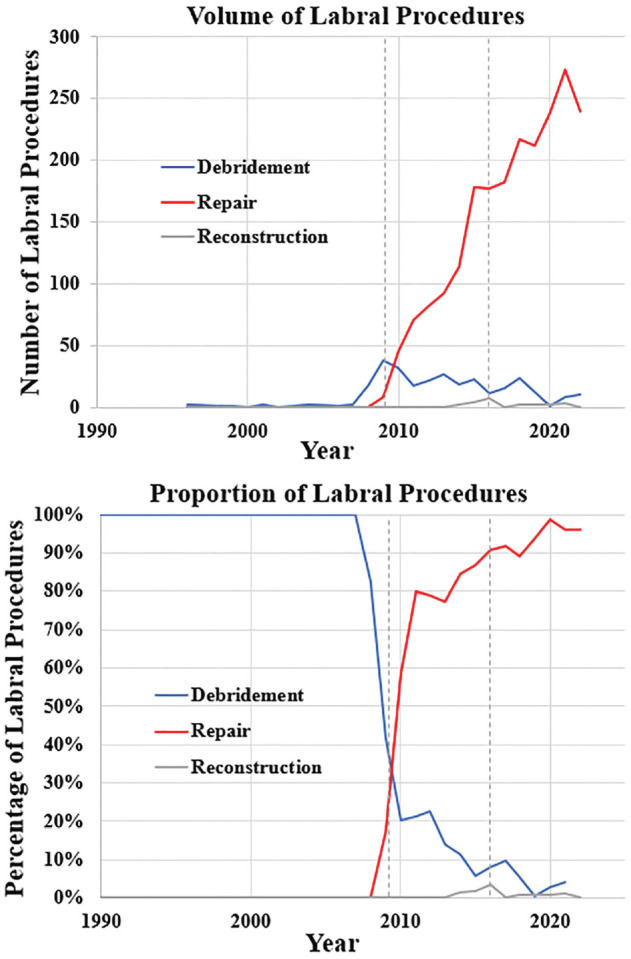
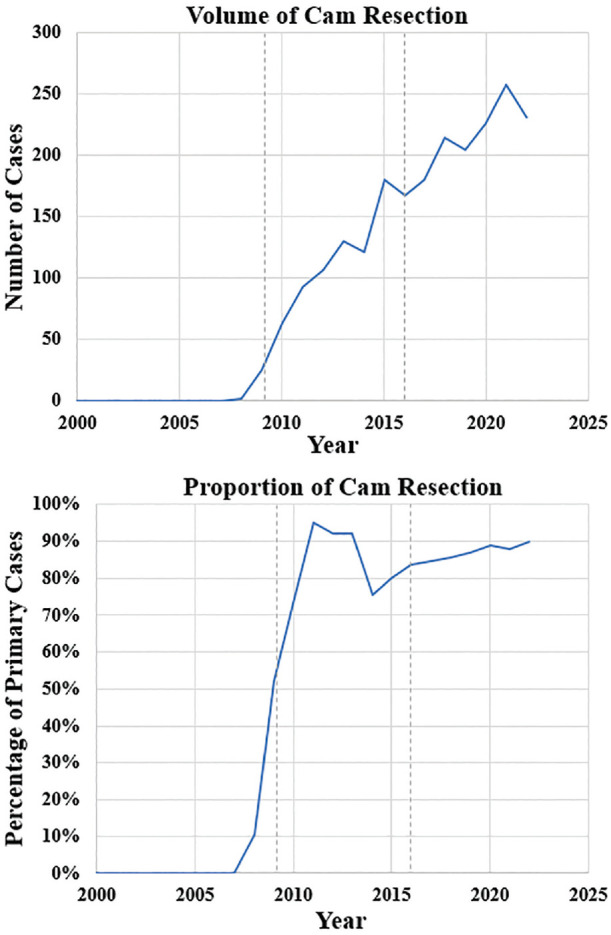
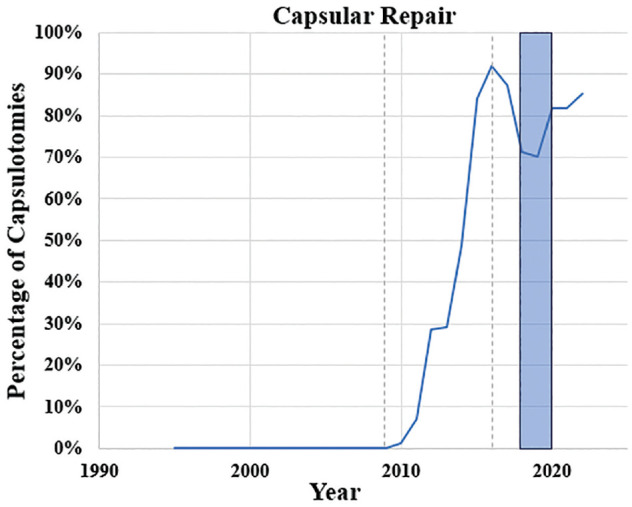
Results: A total of 3000 patients (age, 35.7 ± 13.8 years; age range, 10-89 years; female sex, 2109 (70.3%); body mass index, 27.4 ± 6.3 kg/m2) underwent arthroscopic hip procedures between 1988 and 2022. The mean number of cases increased from a mean of 3.2 per year in 1988-2008 to 285.9 per year in 2016-2022 (P < .001). Labral treatment at the time of primary hip arthroscopy evolved from 100% debridement and 0% repair in 1988-2008 to 5.0% debridement, 94.0% repair, and 1.0% labral reconstruction in 2016-2022 (P < .001). Cam resection increased from 4.1% in 1988-2008 to 86.9% in 2016-2022 (P < .001). By 2022, 45 out of 325 cases (13.8%) were revisions. The rate of capsular repair at the time of primary hip arthroscopy increased from 0.0% in 1988-2008 up to 81.0% in 2016-2022.
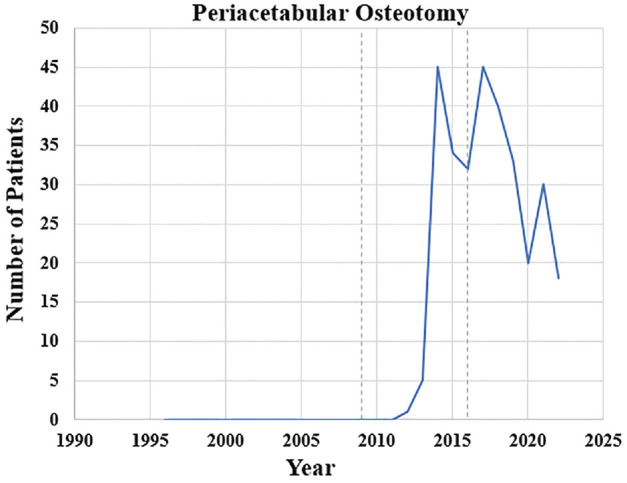
Conclusion: There has been a significant growth of hip arthroscopy volumes as well as a significant transition from use as a tool for diagnosis and labral debridement to procedures restoring native anatomy including labral repair, cam resection, capsular repair, periacetabular osteotomy, and gluteal repair.
Keywords: acetabular labrum repair; cam resection; capsular repair; groin pain; hip arthroscopy; hip/pelvis/thigh; hip: femoroacetabular impingement; osteotomy; pincer resection; psoas fractional lengthening.
© The Author(s) 2024.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: Support from the Foderaro-Quattrone Musculoskeletal-Orthopaedic Surgery Research Innovation Fund. M.M.C. has received education payments from Arthrex and Team 1, consulting fees from Arthrex, and royalties from Arthrex. K.J.E. has received education payments from Goode Surgical and nonconsulting fees from Arthrex. A.J.K. has received a grant from DJO; consulting fees from Arthrex, JRF Ortho, and Responsive Arthroscopy; nonconsulting fees from Arthrex; royalties from Arthrex; and honoraria from JRF Ortho and MTF Biologics. B.A.L. has received consulting fees from Arthrex and Smith & Nephew; nonconsulting fees from Arthrex, Smith & Nephew, and Linvatec; and royalties from Arthrex. M.H. has received financial or material support from Elsevier; education payments from Arthrex, Foundation Medical, Medwest Associates, and Smith & Nephew; consulting fees from Vericel, DJO, and Moximed; royalties from Elsevier; honoraria from Encore Medical; and hospitality payments from Orthalign, Stryker, and Medical Device Business Services. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Bodendorfer BM, Alter TD, Carreira DS, et al.. Multicenter outcomes after primary hip arthroscopy: a comparative analysis of two-year outcomes after labral repair, segmental labral reconstruction, or circumferential labral reconstruction. Arthroscopy. 2022;38(2):352-361. doi:10.1016/j.arthro.2021.05.013 - DOI - PubMed
-
- Burman MS. Arthroscopy or the direct visualization of joints: an experimental cadaver study. J Bone Joint Surg Am. 1931;13(4):669-695. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
