

Neuropathological spectrum of anti-IgLON5 disease and stages of brainstem tau pathology: updated neuropathological research criteria of the disease-related tauopathy
- PMID: 39400557
- PMCID: PMC11473580
- DOI: 10.1007/s00401-024-02805-y
Neuropathological spectrum of anti-IgLON5 disease and stages of brainstem tau pathology: updated neuropathological research criteria of the disease-related tauopathy
Abstract
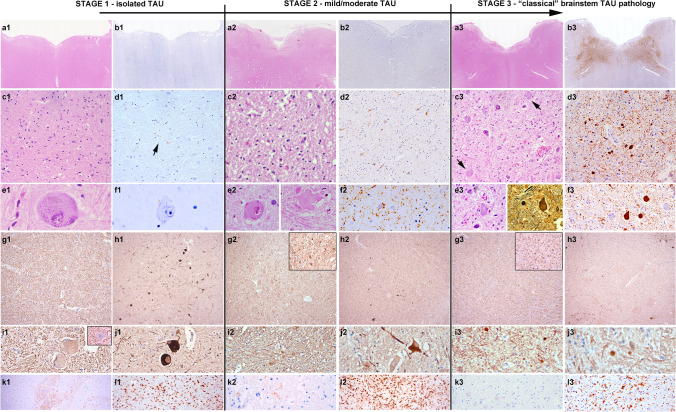
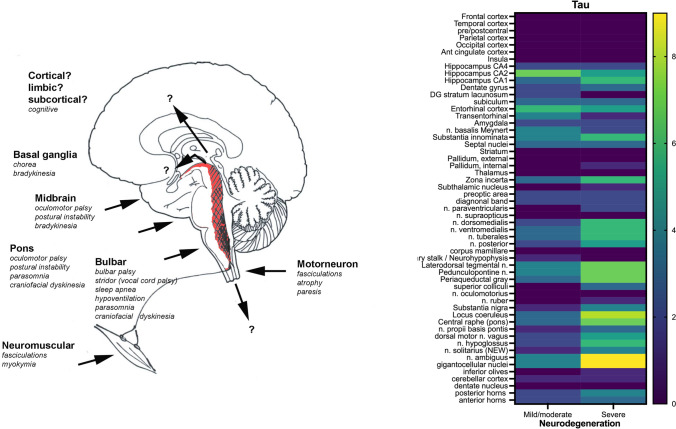
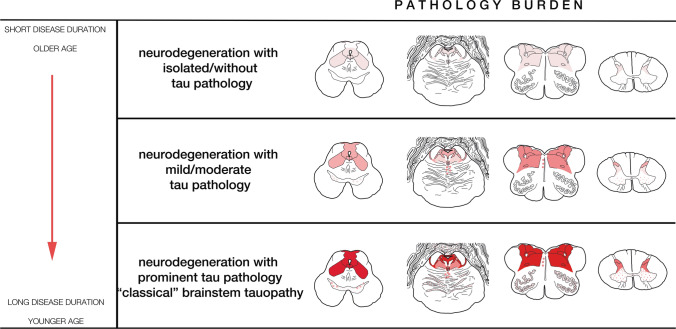
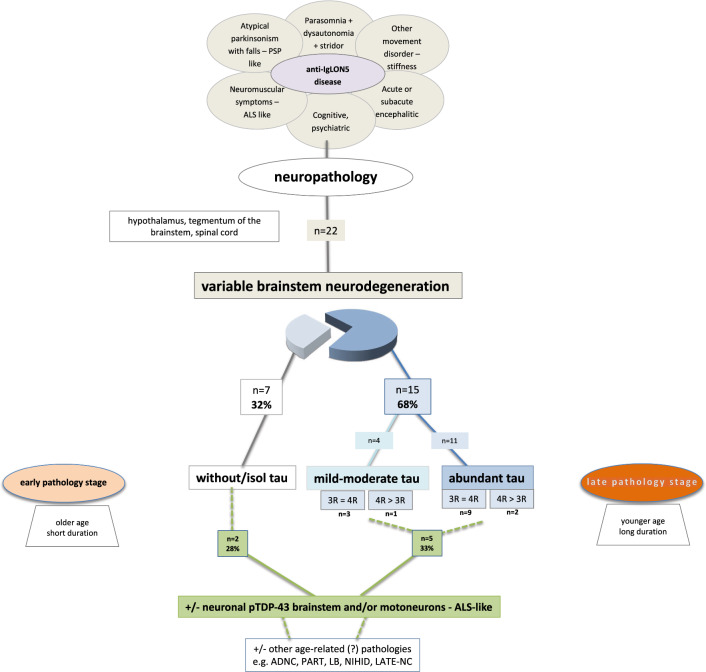
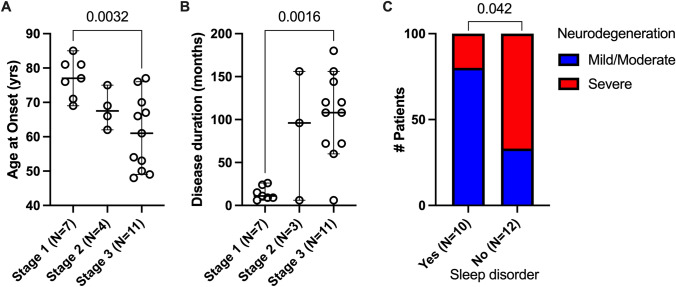
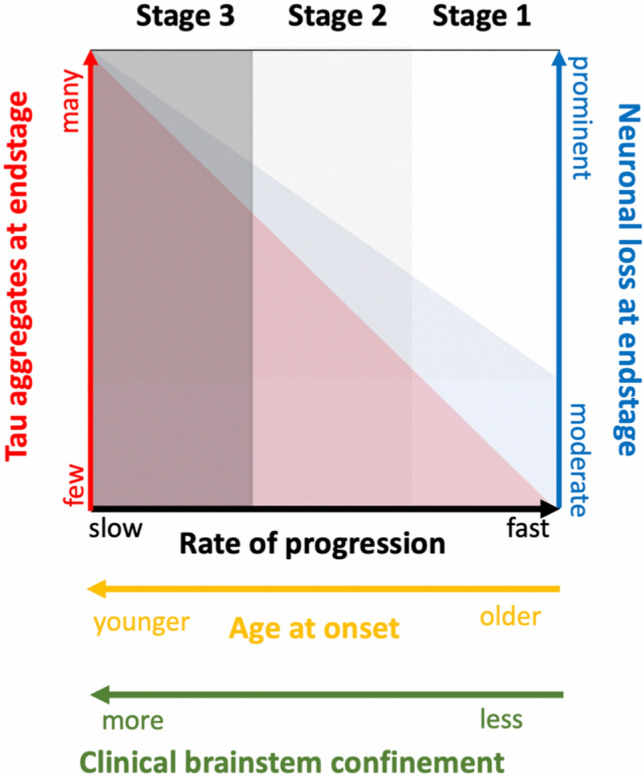
Anti-IgLON5 disease is a unique condition that bridges autoimmunity and neurodegeneration. Since its initial description 10 years ago, an increasing number of autopsies has led to the observation of a broader spectrum of neuropathologies underlying a particular constellation of clinical symptoms. In this study, we describe the neuropathological findings in 22 patients with anti-IgLON5 disease from 9 different European centers. In 15 patients (68%), we observed a hypothalamic and brainstem-predominant tauopathy of varying severity in which the original research neuropathological criteria were readily applicable. This pathology was observed in younger patients (median age at onset 61 years) with a long disease duration (median 9 years). In contrast, in 7 (32%) patients, the originally described brainstem tauopathy was nearly absent or only minimal in the form of delicate threads, despite mild-to-moderate neurodegenerative features, consistent clinical symptoms and the presence of anti-IgLON5 antibodies in CSF and serum. These patients were older at onset (median 79 years) and had shorter disease duration (median < 1 year). Overall, about one-third of the patients showed concomitant TDP-43 pathology within the regions affected by tau pathology and/or neurodegeneration. Based on these observations and in view of the spectrum of the tau burden in the core regions involved in the disease, we propose a simple staging system: stage 1 mild neurodegeneration without overt or only minimal tau pathology, stage 2 moderate neurodegeneration and mild/ moderate tauopathy and stage 3 prominent neurodegeneration and tau pathology. This staging intends to reflect a potential (age- and time-dependent) progression of tau pathology, supporting the current notion that tau accumulation is a secondary phenomenon related to the presence of anti-IgLON5 antibodies in the CNS. Finally, we adapt the original research criteria of the anti-IgLON5 disease-related tauopathy to include the spectrum of pathologies observed in this larger postmortem series.
Keywords: 3R; 4R tau; ALS; Anti-IgLON5 disease; Anti-IgLON5 tauopathy; Atypical; Brainstem tauopathy; Dementia; IgLON5; Motor neuron disease; Neuropathology; PSP; Stages; TDP-43.
© 2024. The Author(s).
Figures
References
-
- Acewicz A, Stępień T, Grzegorczyk M, Ostrowski RP, Tarka S, Felczak P et al (2024) TDP-43 pathology in subacute sclerosing panencephalitis. J Neuropathol Exp Neurol 83:251–257. 10.1093/jnen/nlae017 - PubMed
-
- Alkabie S, Murray BJ, Budhram A (2023) Incidental detection of anti-IgLON5: a diagnostic and therapeutic dilemma. Can J Neurol Sci 26:1–7. 10.1017/cjn.2023.239 - PubMed
-
- Al-Sarraj S, King A, Troakes C, Smith B, Maekawa S, Bodi I et al (2011) p62 positive, TDP-43 negative, neuronal cytoplasmic and intranuclear inclusions in the cerebellum and hippocampus define the pathology of C9orf72-linked FTLD and MND/ALS. Acta Neuropathol 122:691–702. 10.1007/s00401-011-0911-2 - PubMed
-
- Ahmed Z, Josephs KA, Gonzalez J, DelleDonne A, Dickson DW (2008) Clinical and neuropathologic features of progressive supranuclear palsy with severe pallido-nigro-luysial degeneration and axonal dystrophy. Brain 131:460–472. 10.1093/brain/awm301 - PubMed
-
- Askin B, Cordero Gómez C, Lan-Linh Duong S, Kilic C, Goihl A, Newman A et al (2024) Autoimmune antibody-induced neuronal hyperactivity triggers pathological Tau in IgLON5 disease. bioRxiv. 10.1101/2024.03.10.584272
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
