

Progress of nations in the organisation of, and structures for, kidney care delivery between 2019 and 2023: cross sectional survey in 148 countries
- PMID: 39401841
- PMCID: PMC11472216
- DOI: 10.1136/bmj-2024-079937
Progress of nations in the organisation of, and structures for, kidney care delivery between 2019 and 2023: cross sectional survey in 148 countries
Abstract
Objective: To assess changes in key measures of kidney care using data reported in 2019 and 2023.
Design: Cross sectional survey in 148 countries.
Setting: Surveys from International Society of Nephrology Global Kidney Health Atlas between 2019 and 2023 that included participants from countries in Africa (n=36), Eastern and Central Europe (n=16), Latin America (n=18), the Middle East (n=11), Newly Independent States and Russia (n=10), North America and the Caribbean (n=8), North and East Asia (n=6), Oceania and South East Asia (n=15), South Asia (n=7), and Western Europe (n=21).
Participants: Countries that participated in both surveys (2019 and 2023).
Main outcome measures: Comparison of 2019 and 2023 data for availability of kidney replacement treatment services, access, health financing, workforce, registries, and policies for kidney care. Data for countries that participated in both surveys (2019 and 2023) were included in our analysis. Country data were aggregated by International Society of Nephrology regions and World Bank income levels. Proportionate changes in the status of these measures across both periods were reported.
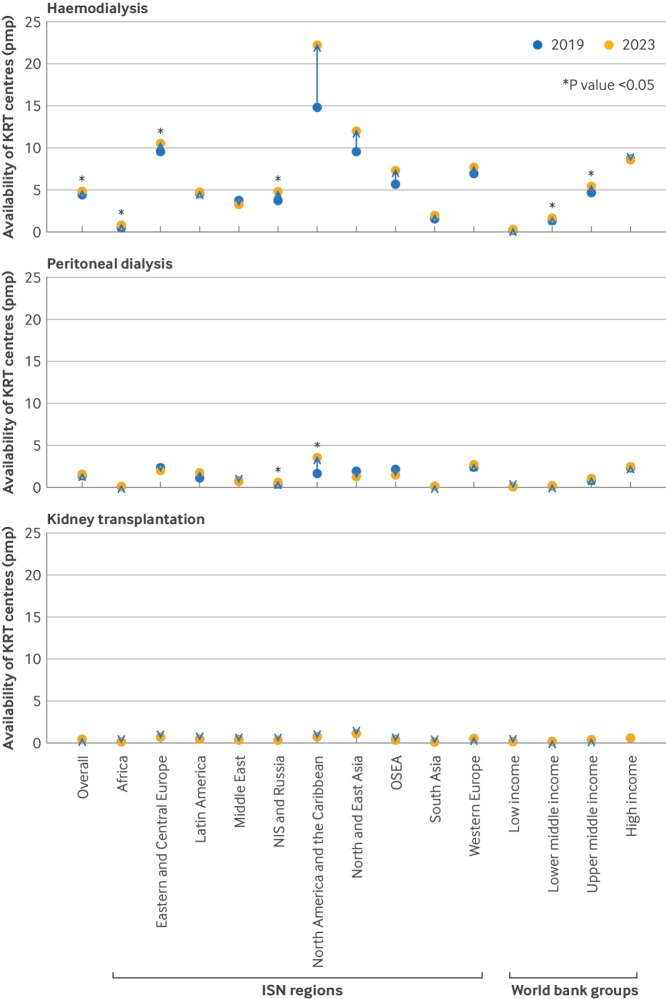
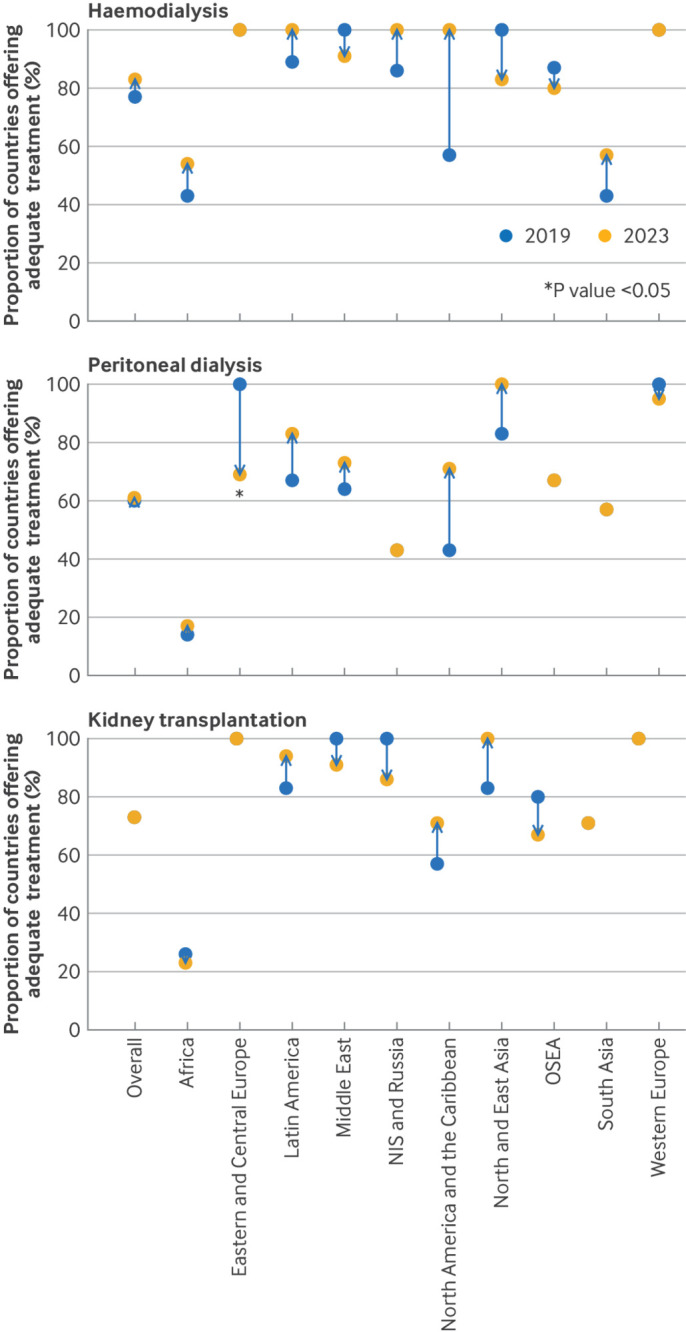
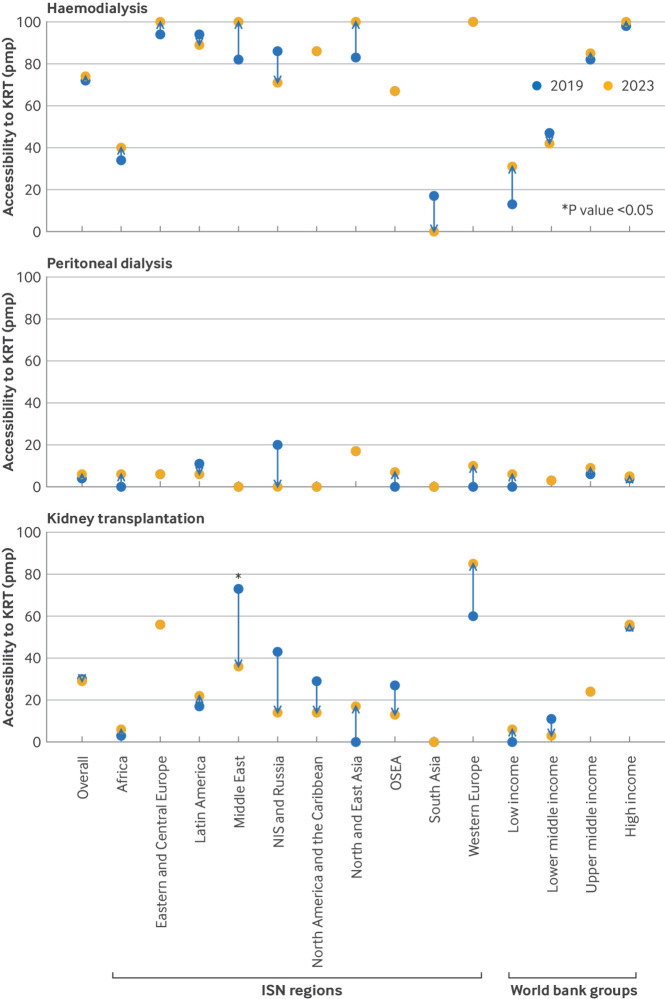
Results: Data for 148 countries that participated in both surveys were available for analysis. The proportions of countries that provided public funding (free at point of delivery) increased from 27% in 2019 to 28% in 2023 for haemodialysis, 23% to 28% for peritoneal dialysis, and 31% to 36% for kidney transplantation services. Centres for these treatments increased from 4.4 per million population (pmp) to 4.8 pmp (P<0.001) for haemodialysis, 1.4 pmp to 1.6 pmp for peritoneal dialysis, and 0.43 pmp to 0.46 pmp for kidney transplantation services. Overall, access to haemodialysis and peritoneal dialysis improved, however, access to kidney transplantation decreased from 30 pmp to 29 pmp. The global median prevalence of nephrologists increased from 9.5 pmp to 12.4 pmp (P<0.001). Changes in the availability of kidney registries and in national policies and strategies for kidney care were variable across regions and country income levels. The reporting of specific barriers to optimal kidney care by countries increased from 55% to 59% for geographical factors, 58% to 68% (P=0.043) for availability of nephrologists, and 46% to 52% for political factors.
Conclusions: Important changes in key areas of kidney care delivery were noted across both periods globally. These changes effected the availability of, and access to, kidney transplantation services. Countries and regions need to enact enabling strategies for preserving access to kidney care services, particularly kidney transplantation.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: funding support for this project from the International Society of Nephrology (grant RES0033080 to the University of Alberta); ST reports fellowship grants from the International Society of Nephrology-Salmasi Family and the Kidney Foundation of Thailand, outside the submitted work. SA reports personal fees from The International Society of Nephrology, outside the submitted work. SD reports personal fees from The International Society of Nephrology, outside the submitted work. JD reports personal fees from The International Society of Nephrology, outside the submitted work. VJ reports personal fees from GSK, Astra Zeneca, Baxter Healthcare, Visterra, Biocryst, Chinook, Vera, and Bayer, paid to his institution, outside the submitted work. VAL reports royalties from Elsevier, consulting fees from the World Health Organization, travel support from the European Renal Association and International Society of Nephrology, and leadership role in Advocacy Working Group of the International Society of Nephrology, outside the submitted work. MN reports grants and personal fees from KyowaKirin, Boehringer Ingelheim, Chugai, Daiichi Sankyo, Torii, Japan Tobacco, Mitsubishi Tanabe, grants from Takeda and Bayer, and personal fees from Astellas, Akebia, AstraZeneca, and GSK, outside the submitted work. AKB reports other (consultancy and honoraria) from AMGEN Incorporated and Otsuka, other (consultancy) from Bayer and GSK, and grants from Canadian Institute of Health Research and Heart and Stroke Foundation of Canada, outside the submitted work; he is also Associate Editor of the Canadian Journal of Kidney Health and Disease and Co-chair of the ISN-Global Kidney Health Atlas. DWJ reports consultancy fees, research grants, speaker’s honoraria and travel sponsorships from Baxter Healthcare and Fresenius Medical Care, consultancy fees from Astra Zeneca, Bayer, and AWAK, speaker’s honoraria from ONO and Boehringer Ingelheim & Lilly, and travel sponsorships from ONO and Amgen, outside the submitted work. He is also a current recipient of an Australian National Health and Medical Research Council Leadership Investigator Grant, outside the submitted work. All other authors have nothing to declare.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical