

Prospective assessment of circulating tumor DNA in patients with metastatic uveal melanoma treated with tebentafusp
- PMID: 39402032
- PMCID: PMC11473804
- DOI: 10.1038/s41467-024-53145-0
Prospective assessment of circulating tumor DNA in patients with metastatic uveal melanoma treated with tebentafusp
Abstract
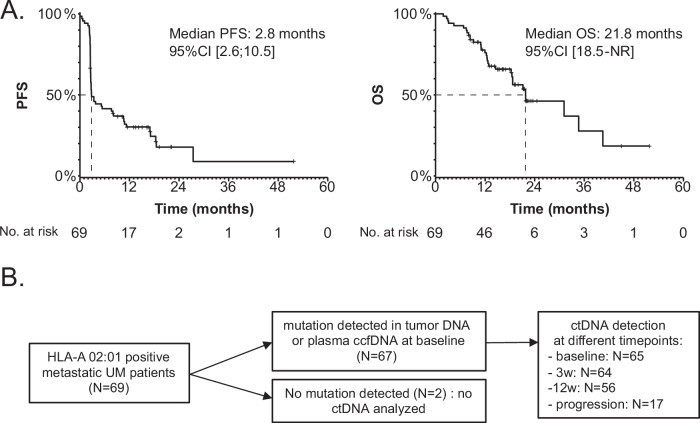
Tebentafusp, a bispecific immune therapy, is the only drug that demonstrated an overall survival benefit in patients with metastatic uveal melanoma (MUM). Circulating tumor DNA (ctDNA) has emerged as a potential prognostic and predictive marker in the phase 3 IMCgp100-202 trial using multiplex PCR-based next-generation sequencing (NGS). In this study (NCT02866149), ctDNA dynamics were assessed using droplet digital PCR (ddPCR) in 69 MUM patients undergoing tebentafusp treatment. Notably, 61% of patients exhibited detectable ctDNA before treatment initiation, which was associated with shorter overall survival (median 12.9 months versus 40.5 months for patients with undetectable ctDNA; p < 0.001). Patients manifesting a 90% or greater reduction in ctDNA levels at 12 weeks demonstrated markedly prolonged overall survival (median 21.2 months versus 12.9 months; p = 0.02). Our findings highlight the potential of ddPCR-based ctDNA monitoring as an economical, pragmatic and informative approach in MUM management, offering valuable insights into treatment response and prognosis.
© 2024. The Author(s).
Conflict of interest statement
M.R. reports personal fees for serving as an advisor from Merck Sharp & Dohme, AstraZeneca, GlaxoSmithKline, Immunocore; travel support from AstraZeneca; funds to his institution to support research from Merck Sharp & Dohme, Janssen-Cilag, Daiichi-Sankyo. F-C.B. received advisory board fees from Pfizer, AstraZeneca, Daiichi-Sankyo, Lilly, Novartis, Menarini, Caris Life Science, GE Healthcare, Exact Sciences, Gilead, Roche, SAGA Diagnostics; research support from AstraZeneca, Novartis, Pfizer, Prolynx, Merck KGAa, GE Healthcare, SAGA Diagnostics, Personalis; travel support from AstraZeneca, Novartis, Pfizer, Daiichi-Sankyo. A.V-S. received research grant from AstraZeneca, Daiichi-Sankyo, Ibex, Owkin, Primaa; travel support from AstraZeneca, Roche; conference fees from Daiichi-Sankyo, Exactsciences, Amgen; honoraria for conferences or lectures from AstraZeneca, Roche, MSD, Exactsciences; advisory board or consultant fees from Ibex, Primaa. M.P. received advisory board fees and travel support from AstraZeneca. J-E.K. reports personal fees for serving as an advisor from GlaxoSmithKline, Clovis Oncology, Tesaro, AstraZeneca, and Dragonfly Therapeutics; funds to his institution to support research from Merck Sharp & Dohme; travel support from Roche, PharmaMar, Tesaro. S.P-N reports personal fees for serving as an advisor from Immunocore and Pierre Fabre and travel support from Immunocore, Novartis. M-H.S. and S.R. received research support from Immunocore. The remaining authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
