

Combined associations of physical activity, diet quality and their changes over time with mortality: findings from the EPIC-Norfolk study, United Kingdom
- PMID: 39402526
- PMCID: PMC11476187
- DOI: 10.1186/s12916-024-03668-6
Combined associations of physical activity, diet quality and their changes over time with mortality: findings from the EPIC-Norfolk study, United Kingdom
Abstract
Background: Physical activity (PA) and diet quality have each been shown to be inversely associated with mortality but their combined impact on longevity has been less explored, particularly when considering their changes over time. This study aimed to examine the separate and combined associations of PA, diet quality and their changes over time with mortality outcomes.
Methods: A prospective cohort study was performed on 9349 adults aged 40 to 79 years from the population-based European Prospective Investigation into Cancer in Norfolk Study, with repeated measurements of PA and diet (from 1993 till 2004) and subsequent follow-up till 2022 (median follow-up 18.8 years). Validated questionnaires were used to derive physical activity energy expenditure (PAEE) as a proxy of total PA and adherence to the Mediterranean diet score (MDS, range 0-15 points) as an indicator of overall diet quality, and their changes over time (∆PAEE and ∆MDS). Cox regression models adjusted for potential confounders and mediators were used to estimate hazard ratios (HRs) and 95% CIs.
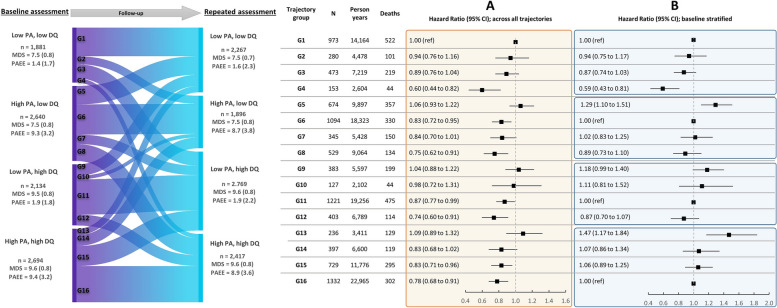
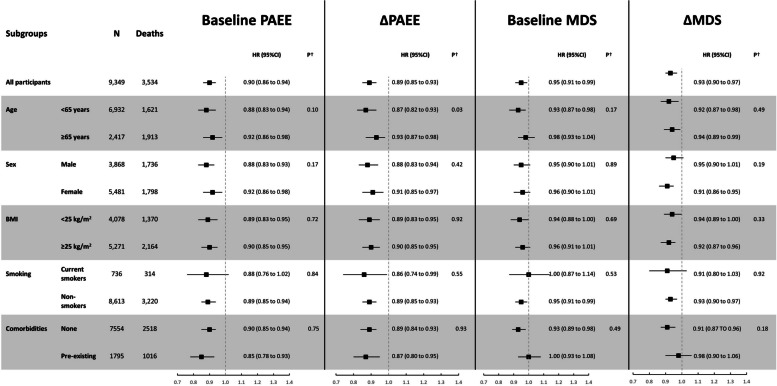
Results: Over 149,681 person-years of follow-up, there were 3534 deaths. In adjusted models, for each 1-SD difference in baseline PAEE (4.64 kJ/kg/day), ∆PAEE (0.65 kJ/kg/day per year), baseline MDS (1.30 points) and ∆MDS (0.32 points per year), HRs (95% CI) for all-cause mortality were 0.90 (0.86 to 0.94), 0.89 (0.85 to 0.93), 0.95 (0.91 to 0.99) and 0.93 (0.90 to 0.97), respectively. Compared with participants with sustained low PAEE (< 5 kJ/kg/day) and low MDS (< 8.5 points), those with sustained high PAEE and high MDS had lower all-cause mortality (HR 0.78; 95% CI: 0.68-0.91), as did those who improved both PAEE and MDS (0.60; 0.44-0.82). There was no evidence of interaction between PA and diet quality exposures on mortality risk. Population impact estimates suggested that if all participants had maintained high levels of PA and diet quality consistently, cumulative adjusted mortality rate would have been 8.8% (95% CI: 2.4 to 15.3%) lower.
Conclusions: These findings suggest that adopting and maintaining higher levels of PA and diet quality are associated with lower mortality. Significant public health benefits could be realised by enabling active living and healthy eating through adulthood.
Keywords: Cancer mortality; Cardiovascular diseases mortality; Cohort studies; Diet quality; Mediterranean diet; Mortality; Physical activity; Prospective studies; Trajectories.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Rosato V, Temple NJ, La Vecchia C, Castellan G, Tavani A, Guercio V. Mediterranean diet and cardiovascular disease: a systematic review and meta-analysis of observational studies. Eur J Nutr. 2019;58(1):173–91. - PubMed
-
- Becerra-Tomás N, Blanco Mejía S, Viguiliouk E, Khan T, Kendall CWC, Kahleova H, et al. Mediterranean diet, cardiovascular disease and mortality in diabetes: a systematic review and meta-analysis of prospective cohort studies and randomized clinical trials. Crit Rev Food Sci Nutr. 2020;60(7):1207–27. - PubMed
-
- Eleftheriou D, Benetou V, Trichopoulou A, La Vecchia C, Bamia C. Mediterranean diet and its components in relation to all-cause mortality: meta-analysis. Br J Nutr. 2018;120(10):1081–97. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
