

Association between stress hyperglycemia ratio index and all-cause mortality in critically ill patients with atrial fibrillation: a retrospective study using the MIMIC-IV database
- PMID: 39402588
- PMCID: PMC11476318
- DOI: 10.1186/s12933-024-02462-1
Association between stress hyperglycemia ratio index and all-cause mortality in critically ill patients with atrial fibrillation: a retrospective study using the MIMIC-IV database
Abstract
Background: The stress hyperglycemia ratio (SHR) was developed to mitigate the influence of long-term chronic glycemic factors on stress hyperglycemia levels, which are associated with adverse clinical events, particularly cardiovascular events. However, studies examining the SHR index and its prognostic significance in patients with atrial fibrillation (AF) are lacking. This study aims to evaluate the relationship between the SHR index and all-cause mortality in critically ill patients with AF upon Intensive Care Unit admission.
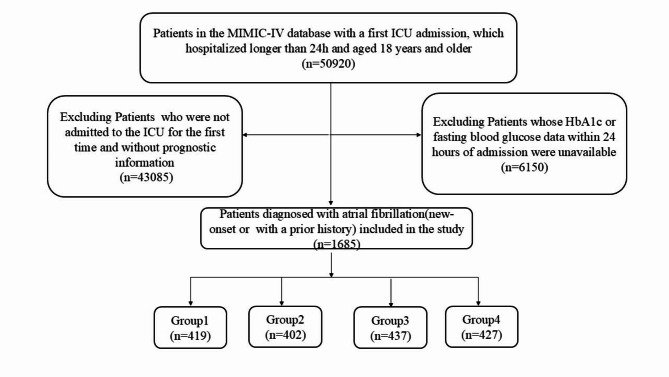
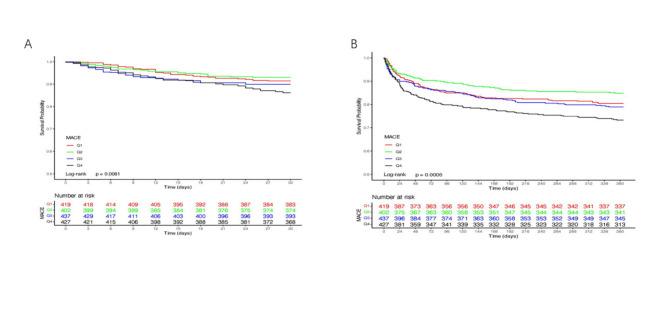
Methods: The patients' data were extracted from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database. All patients were categorized into four groups based on the SHR index. The outcomes include both primary and secondary endpoints, with the primary endpoints being 30-day and 365-day all-cause mortality, and the secondary endpoints being 90-day and 180-day all-cause mortality. The SHR index was analyzed using quartiles, and the Kaplan-Meier curve was employed to compare the outcomes across groups. Cox proportional-hazards regression and restricted cubic splines (RCS) were used to assess the relationship between the SHR index and the outcomes.
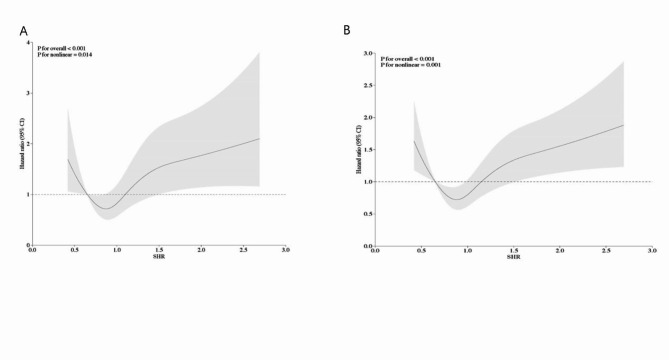
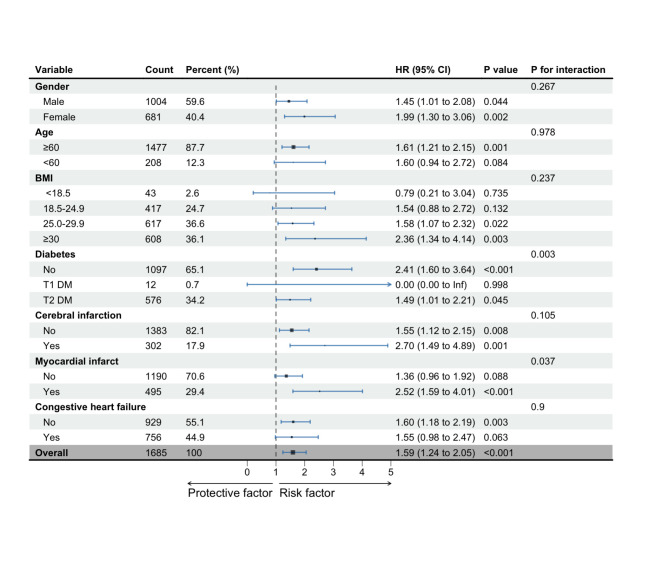
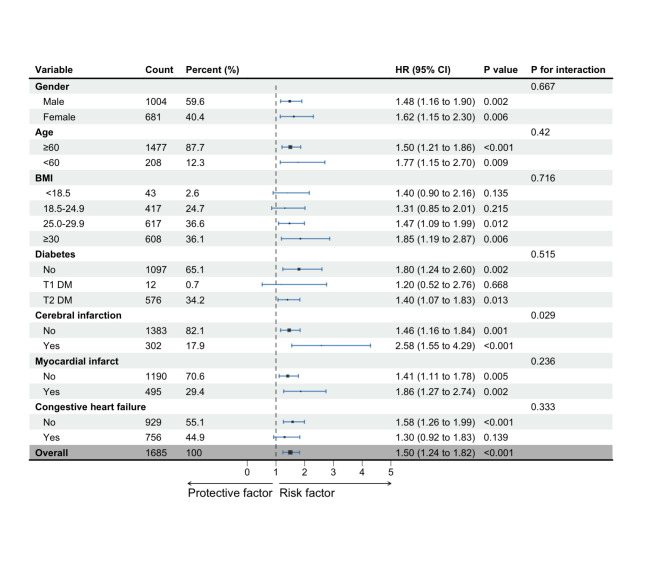
Results: Out of a total of 1,685 participants, the average age was 63.12 years (range: 40.17 to 101.49), with 1,004 (59.58%) being male. Higher levels of the SHR index were associated with an increased risk of all-cause mortality at 30 days, 90 days, 180 days, and 365 days, as indicated by the Kaplan-Meier curves (log-rank P < 0.01). Additionally, Cox proportional-hazards regression analysis revealed that the risk of mortality at these time points was significantly higher in the highest quartile of the SHR index. Restricted cubic splines (RCS) analysis demonstrated U-shaped relationships between the SHR index and all-cause mortality, with inflection points at 0.73 for 30-day mortality and 0.76 for 365-day mortality. Compared to patients with SHR levels below these inflection points, those with higher levels had a 69.9% increased risk for 30-day all-cause mortality (hazard ratio [HR] 1.699; 95% confidence interval [CI] 1.336 to 2.159) and a 61.6% increased risk for 365-day all-cause mortality (HR 1.616; 95% CI 1.345 to 1.942).
Conclusion: In critically ill patients with AF, higher levels of the SHR index are significantly associated with an increased risk of all-cause mortality at 30 days, 90 days, 180 days, and 365 days. The SHR index may serve as a valid indicator for assessing the severity and guiding the treatment of AF patients in the ICU.
Keywords: All-cause mortality; Atrial fibrillation; Prognosis; Stress hyperglycemia ratio.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Stress hyperglycemia ratio and machine learning model for prediction of all-cause mortality in patients undergoing cardiac surgery.Cardiovasc Diabetol. 2025 Feb 15;24(1):77. doi: 10.1186/s12933-025-02644-5. Cardiovasc Diabetol. 2025. PMID: 39955587 Free PMC article.
-
Association between trajectory of triglyceride-glucose index and all-cause mortality in critically ill patients with atrial fibrillation: a retrospective cohort study.Cardiovasc Diabetol. 2025 Jul 10;24(1):278. doi: 10.1186/s12933-025-02838-x. Cardiovasc Diabetol. 2025. PMID: 40640797 Free PMC article.
-
Combined assessment of stress hyperglycemia ratio and glycemic variability to predict all-cause mortality in critically ill patients with atherosclerotic cardiovascular diseases across different glucose metabolic states: an observational cohort study with machine learning.Cardiovasc Diabetol. 2025 May 9;24(1):199. doi: 10.1186/s12933-025-02762-0. Cardiovasc Diabetol. 2025. PMID: 40346649 Free PMC article.
-
Association between triglyceride-glucose index and mortality in critically ill patients with atrial fibrillation: a retrospective cohort study.Cardiovasc Diabetol. 2025 Mar 24;24(1):138. doi: 10.1186/s12933-025-02697-6. Cardiovasc Diabetol. 2025. PMID: 40128768 Free PMC article.
-
The association between the stress hyperglycaemia ratio and mortality in cardiovascular disease: a meta-analysis and systematic review.Cardiovasc Diabetol. 2024 Nov 16;23(1):412. doi: 10.1186/s12933-024-02454-1. Cardiovasc Diabetol. 2024. PMID: 39550575 Free PMC article.
Cited by
-
Stress hyperglycemia ratio as a biomarker for early mortality risk stratification in cardiovascular disease: a propensity-matched analysis.Cardiovasc Diabetol. 2025 Jul 12;24(1):286. doi: 10.1186/s12933-025-02812-7. Cardiovasc Diabetol. 2025. PMID: 40652236 Free PMC article.
-
Predictive performance of stress hyperglycemia ratio for poor prognosis in critically ill patients: a systematic review and dose-response meta-analysis.Eur J Med Res. 2025 Jul 11;30(1):613. doi: 10.1186/s40001-025-02868-x. Eur J Med Res. 2025. PMID: 40646634 Free PMC article. Review.
-
The association between the lactate to albumin ratio and all-cause mortality in cardiac arrest patients: an analysis of the MIMIC-IV database.Eur J Med Res. 2025 Aug 5;30(1):712. doi: 10.1186/s40001-025-02986-6. Eur J Med Res. 2025. PMID: 40765007 Free PMC article.
-
Association between the (neutrophil + monocyte)/albumin ratio and all-cause mortality in sepsis patients: a retrospective cohort study and predictive model establishment according to machine learning.BMC Infect Dis. 2025 Apr 22;25(1):579. doi: 10.1186/s12879-025-10969-5. BMC Infect Dis. 2025. PMID: 40264028 Free PMC article.
-
Unveiling the role of stress hyperglycemia in predicting mortality for critically ill hemorrhagic stroke patients: insights from MIMIC-IV.Front Endocrinol (Lausanne). 2025 May 2;16:1558352. doi: 10.3389/fendo.2025.1558352. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40385356 Free PMC article.
References
-
- Hindricks G, Potpara T, Dagres N et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021,42(5):373–498. 10.1093/eurheartj/ehaa612 - PubMed
-
- AI-Khatib S. Atrial fibrillation. Ann Intern Med. 2023;176(7):ITC97–112. 10.7326/AITC202307180. - PubMed
-
- Wetterslev M, Haase N, Hassager C, et al. New-onset atrial fibrillation in adult critically ill patients: a scoping review. Intensive Care Med. 2019;45(7):928–38. 10.1007/s00134-019-05633-x. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
