

Comprehensive biomarker and modeling approach to support dose finding for BI 836880, a VEGF/Ang-2 inhibitor
- PMID: 39402675
- PMCID: PMC11476076
- DOI: 10.1186/s12967-024-05612-x
Comprehensive biomarker and modeling approach to support dose finding for BI 836880, a VEGF/Ang-2 inhibitor
Abstract
Background: BI 836880 is a humanized bispecific nanobody® that binds to and blocks vascular endothelial growth factor (VEGF) and angiopoietin-2 (Ang-2). A comprehensive biomarker and modeling approach is presented here that supported dose finding for BI 836880.
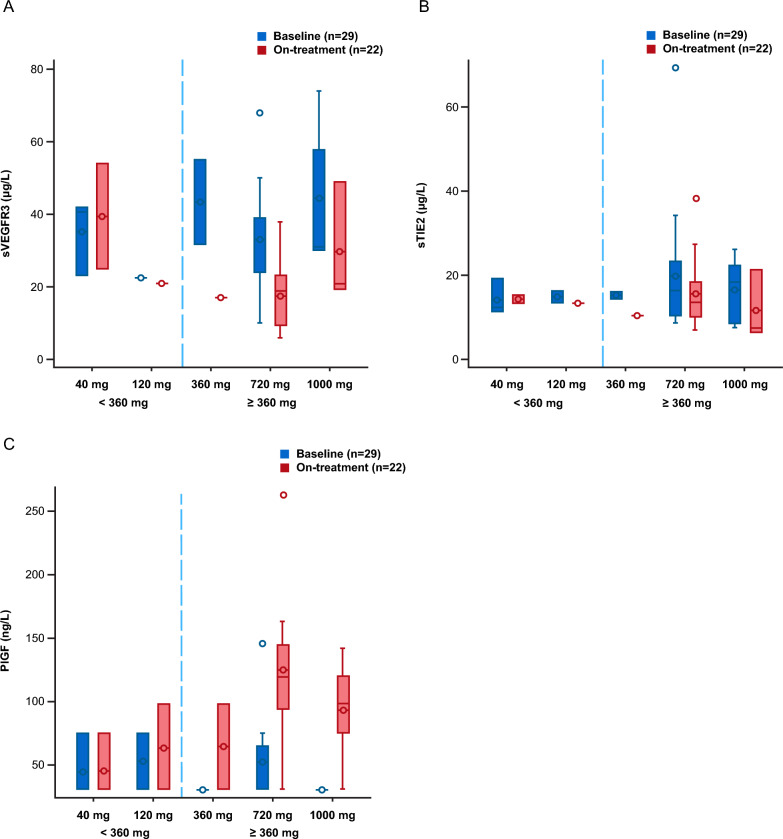
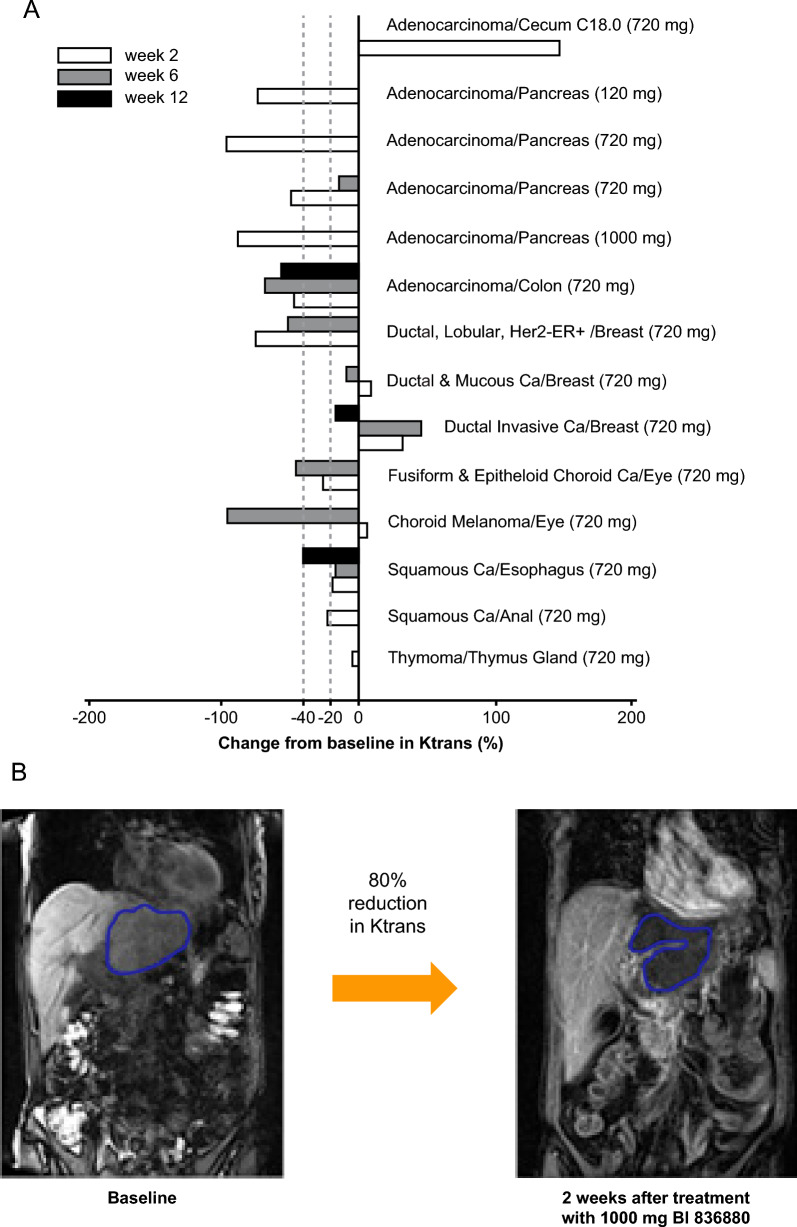
Methods: Two Phase I dose-escalation studies (1336.1 [NCT02674152], 1336.6 [NCT02689505]) assessed BI 836880 in adults with confirmed locally advanced or metastatic solid tumors, refractory to standard therapy or for which standard therapy was not reliably effective. Two dosing schedules were investigated, 3 weeks (q3w) or once weekly (qw), starting at a dose of 40 mg. In a comprehensive biomarker approach, soluble pharmacodynamic markers (free and total plasma VEGF-A and Ang-2), as well as circulating angiogenic factors (soluble VEGF3, soluble Tie2 and placenta growth factor, amongst others) were analyzed to assess target engagement in peripheral blood for q3w doses. A Population based pharmacokinetics/pharmacodynamics (PopPK/PD) model was built using the limited Phase I dataset to support dose finding by simulations. In order to demonstrate drug activity in the tumor, dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) was applied.
Results: DCE-MRI scans supported target engagement in the tumor. Free VEGF-A was depleted at all doses, whereas free Ang-2 decreased dose-dependently, reaching depletion in most patients from 360 mg q3w onwards. While total VEGF-A levels increased in a dose-dependent manner, reaching saturation at 360 mg q3w, total Ang-2 levels increased, but did not plateau. Angiogenic biomarkers showed changes from doses ≥ 360 mg q3w. PopPK/PD modeling showed that doses ≥ 360 mg q3w led to > 90% inhibition of free Ang-2 at steady-state in most patients. By increasing the dose to ≥ 500 mg q3w, > 90% of patients are expected to achieve this level.
Conclusions: The comprehensive analyses of multiple target engagement markers support BI 836880 720 mg q3w as a biologically relevant monotherapy dose schedule.
Trial registration: NCT02674152 and NCT02689505.
Keywords: Ang-2; BI 836880; Biomarkers; Pharmacodynamics; Pharmacokinetics; VEGF.
© 2024. The Author(s).
Conflict of interest statement
S Keller, U Kunz, U Schmid, M He, G Jayadeva, D Luedtke, HG. Niessen, Z Oum’Hamed, S Pleiner and R Graeser are or have all been employees of Boehringer Ingelheim. J Beusmans and X Wang are employees of Metrum Research Group. M Büchert and C Le Tourneau declare no competing interests.
Figures

References
-
- World Health Organization. Global cancer burden growing, amidst mounting need for services. https://www.who.int/news/item/01-02-2024-global-cancer-burden-growing--a.... Accessed 07 Aug 2024. - PMC - PubMed
-
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–63. 10.3322/caac.21834. - PubMed
-
- Anand U, Dey A, Chandel AKS, Sanyal R, Mishra A, Pandey DK, De Falco V, Upadhyay A, Kandimalla R, Chaudhary A, Dhanjal JK, Dewanjee S, Vallamkondu J, de la Lastra JMP. Cancer chemotherapy and beyond: current status, drug candidates, associated risks and progress in targeted therapeutics. Genes Dis. 2023;10:1367–401. 10.1016/j.gendis.2022.02.007. - PMC - PubMed
-
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144:646–74. 10.1016/j.cell.2011.02.013. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
