

Neurodevelopmental predictors of treatment response in schizophrenia and bipolar disorder
- PMID: 39402801
- PMCID: PMC11536111
- DOI: 10.1017/S0033291724001776
Neurodevelopmental predictors of treatment response in schizophrenia and bipolar disorder
Abstract
Background: Treatment resistance is a major challenge in psychiatric disorders. Early detection of potential future resistance would improve prognosis by reducing the delay to appropriate treatment adjustment and recovery. Here, we sought to determine whether neurodevelopmental markers can predict therapeutic response.
Methods: Healthy controls (N = 236), patients with schizophrenia (N = 280) or bipolar disorder (N = 78) with a known therapeutic outcome, were retrospectively included. Age, sex, education, early developmental abnormalities (obstetric complications, height, weight, and head circumference at birth, hyperactivity, dyslexia, epilepsy, enuresis, encopresis), neurological soft signs (NSS), and ages at first subjective impairment, clinical symptoms, treatment, and hospitalization, were recorded. A supervised algorithm leveraged NSS and age at first clinical signs to classify between resistance and response in schizophrenia.
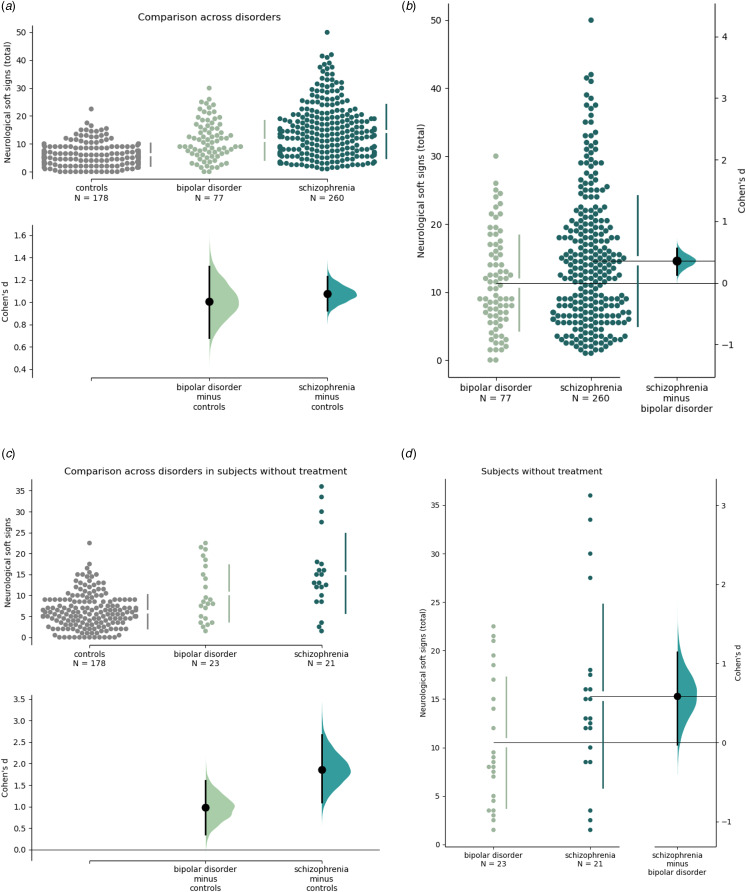
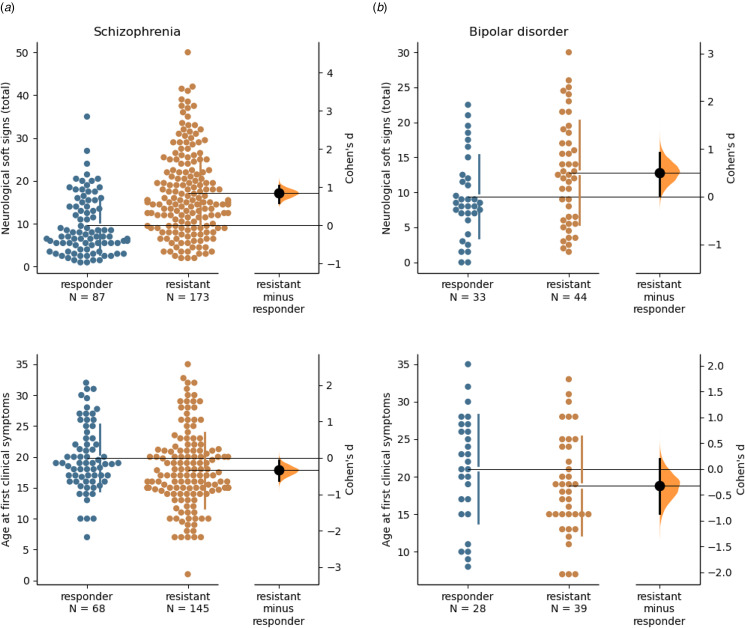
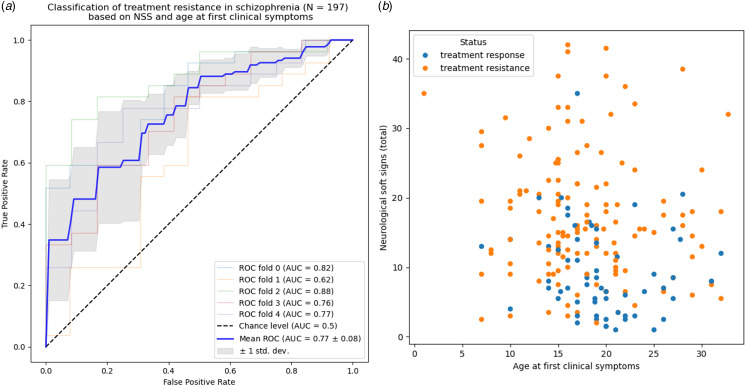
Results: Developmental abnormalities were more frequent in schizophrenia and bipolar disorder than in controls. NSS significantly differed between controls, responsive, and resistant participants with schizophrenia (5.5 ± 3.0, 7.0 ± 4.0, 15.0 ± 6.0 respectively, p = 3 × 10-10) and bipolar disorder (5.5 ± 3.0, 8.3 ± 3.0, 12.5 ± 6.0 respectively, p < 1 × 10-10). In schizophrenia, but not in bipolar disorder, age at first subjective impairment was three years lower, and age at first clinical signs two years lower, in resistant than responsive subjects (p = 2 × 10-4 and p = 9 × 10-3, respectively). Age at first clinical signs and NSS accurately predicted treatment response in schizophrenia (area-under-curve: 77 ± 8%, p = 1 × 10-14).
Conclusions: Neurodevelopmental features such as NSS and age of clinical onset provide a means to identify patients who may require rapid treatment adaptation.
Keywords: age at onset of disease; bipolar disorder; neurodevelopment; neurological soft signs; schizophrenia; treatment response.
Conflict of interest statement
The authors report no conflict of interest in relation to this work.
Figures
References
-
- Ajnakina, O., Das, T., Lally, J., Di Forti, M., Pariante, C. M., Marques, T. R., … Dazzan, P. (2021). Structural covariance of cortical gyrification at illness onset in treatment resistance: A longitudinal study of first-episode psychoses. Schizophrenia Bulletin, 47(6), 1729–1739. doi: 10.1093/schbul/sbab035 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
