

Prescribed cumulative dosage of corticosteroids to patients with inflammatory bowel disease diagnosed between 2006 and 2020: a retrospective observational study
- PMID: 39403301
- PMCID: PMC11472373
- DOI: 10.1177/17562848241288851
Prescribed cumulative dosage of corticosteroids to patients with inflammatory bowel disease diagnosed between 2006 and 2020: a retrospective observational study
Abstract
Background: Treatments and strategies for inflammatory bowel disease (IBD) have gradually evolved in the 2000s.
Objectives: We investigated whether the prescription of corticosteroids (prednisolone and budesonide) in patients with IBD in the first 5 years after diagnosis changed in patients diagnosed between 2006 and 2018.
Design: Retrospective observational study.
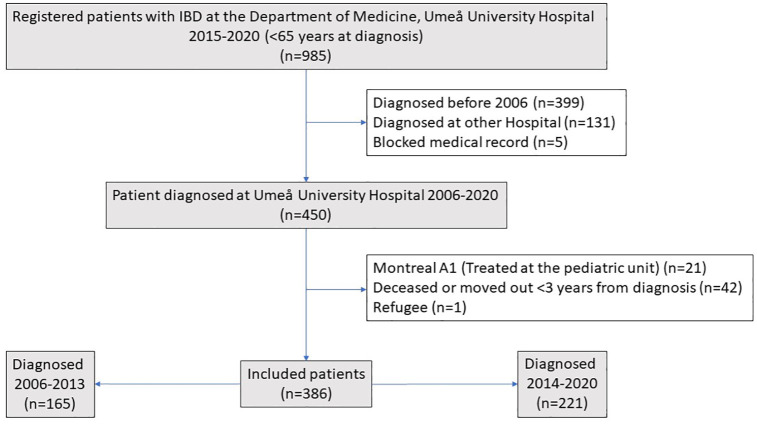
Methods: The cumulative prescribed dosage of corticosteroids for the first 5 years after diagnosis was registered in all patients with IBD (n = 386) at our clinic for those diagnosed between 2006 and 2018.
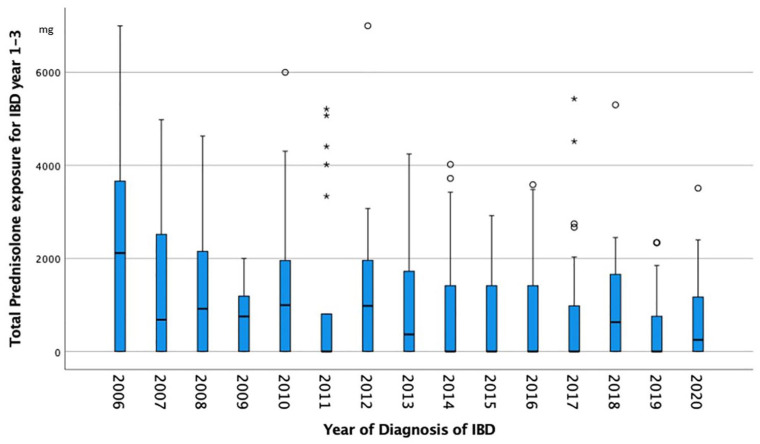
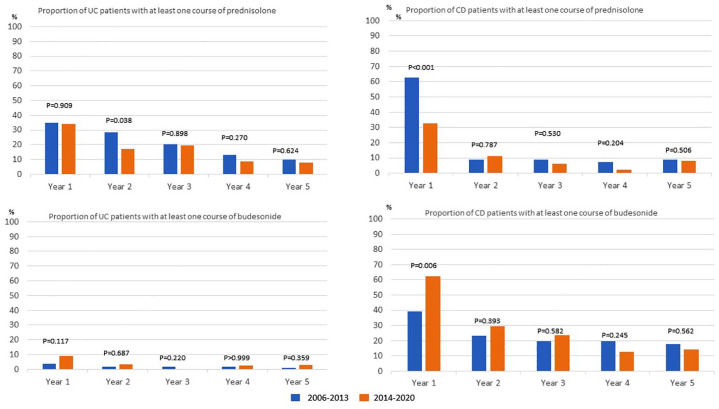
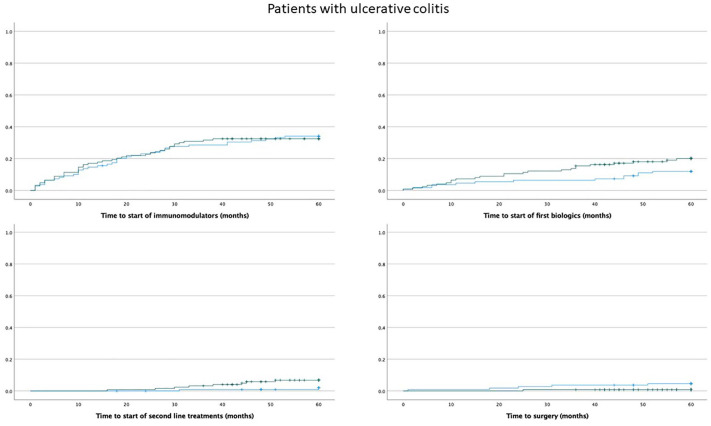
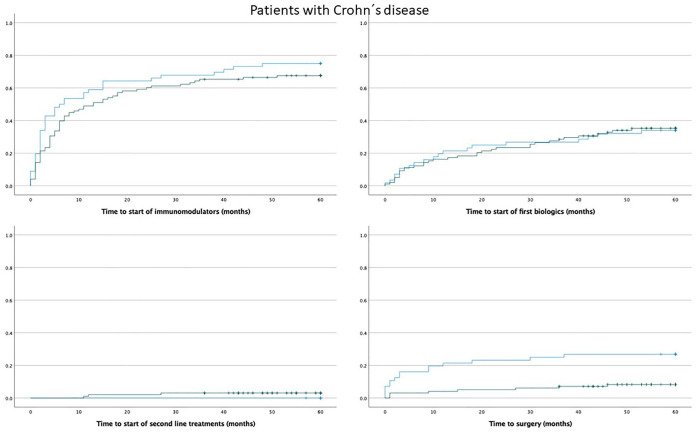
Results: The proportion of patients with IBD who were prescribed at least one prescription of corticosteroids in year 1-5 after diagnosis was 55.3%, 27.9%, 22.7%, 14.1%, and 14.6%, respectively. The proportion of patients who had a cumulative dose of prednisolone >1 g in the first 5 years after diagnosis was 40.1% for ulcerative colitis and 34.9% for Crohn's disease (CD). The cumulative prescribed dosage (within 3 years after diagnosis) of prednisolone had declined (rs = -0.164, p = 001), but had increased for budesonide (rs = 0.202, p < 0.001) between 2006 and 2020. The prescription of any immunomodulator for IBD in the first 5 years from diagnosis was stable between 2006 and 2018 (rs = 0.056, p = 0.257), but there was a minor increase in the prescription of Tumor Necrosis Factor (TNF)-inhibitors (rs = 0.119, p = 0.020). The use of five-acetyl salicylic acid (5-ASA) decreased in patients with CD (rs = -201, p = 0.012).
Conclusion: There was a decrease in the prescription of prednisolone and an increase in the prescription of budesonide treatment from 2006 to 2023; however, the cumulative exposure to corticosteroids in patients with IBD remains at a relatively high level.
Keywords: 5-ASA; Crohn’s disease; biologics; budesonide; immunomodulators; inflammatory bowel disease; prednisolone; surgery; ulcerative colitis.
Plain language summary
The use of steroids in patients with inflammatory bowel disease diagnosed between 2006 and 2020 In the 1950s, corticosteroids and immunomodulators were introduced, and in combination with improved surgery, the mortality rates dramatically decreased in patients with inflammatory bowel disease (IBD) Although corticosteroids are effective in the short term they have no proven efficacy in long-term therapy for IBD, and owing to the risk of side effects, their long-term use should be restricted. Based on the evolution of treatments and treatment strategies for IBD in the 2000s, we aimed to study to the extent to which corticosteroids have been used in the first five years after diagnosis for patients with IBD diagnosed at our clinic between 2006 and 2020. To what extent is prednisolone prescribed in the first five years after diagnosis? Has the pattern of corticosteroid prescription changed after the introduction of advanced therapy and biosimilars to TNF inhibitors? We found that the proportion of patients with IBD who were prescribed at least one prescription of corticosteroids in year one to five after diagnosis was 55.3%, 27.9%, 22.7%, 14.1%, and 14.6%, respectively. The proportion of patients who had a cumulative dose of prednisolone >1g in the first five years after diagnosis was 40.1% for ulcerative colitis (UC) and 34.9% for Crohns disease (CD). The cumulative prescribed dosage (within 3 years after diagnosis) of prednisolone had declined but increased for budesonide between 2006-2020. The prescription of any immunomodulator for IBD in the first five years from diagnosis was stable between the years 2006-2018, but there was a minor increase in the prescription of TNF-inhibitors. The use of 5-ASA decreased in patients with CD. We conclude that there was a decrease in the prescription of prednisolone and an increase in the prescription of budesonide treatment from 2006 to 2023; however, the cumulative exposure to corticosteroids in patients with IBD remains on relatively high level.
© The Author(s), 2024.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Kirsner JB. Historical origins of medical and surgical therapy of inflammatory bowel disease. Lancet 1998; 352: 1303–1305. - PubMed
-
- Ford AC, Bernstein CN, Khan KJ, et al. Glucocorticosteroid therapy in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol 2011; 106: 590–599; quiz 600. - PubMed
-
- Benchimol EI, Seow CH, Otley AR, et al. Budesonide for maintenance of remission in Crohn’s disease. Cochrane Database Syst Rev 2009; 2009: CD002913. - PubMed
-
- Lennard-Jones JE, Misiewicz JJ, Connell AM, et al. Prednisone as maintenance treatment for ulcerative colitis in remission. Lancet 1965; 1: 188–189. - PubMed
LinkOut - more resources
Full Text Sources
