

Case report: Fatal hemoptysis after effective treatment with tislelizumab and anlotinib in pulmonary sarcomatoid carcinoma
- PMID: 39403337
- PMCID: PMC11471433
- DOI: 10.3389/fonc.2024.1445358
Case report: Fatal hemoptysis after effective treatment with tislelizumab and anlotinib in pulmonary sarcomatoid carcinoma
Abstract
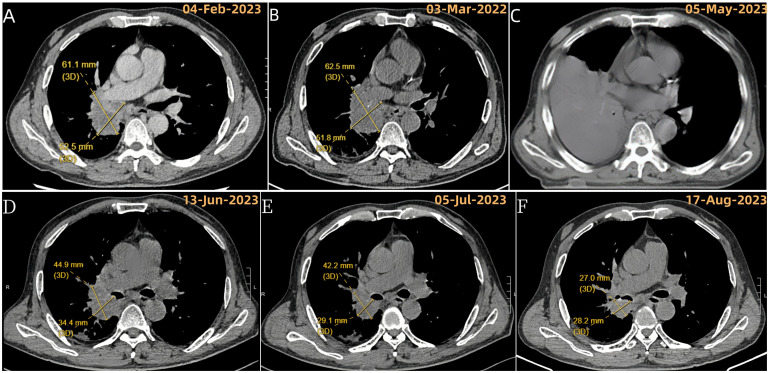
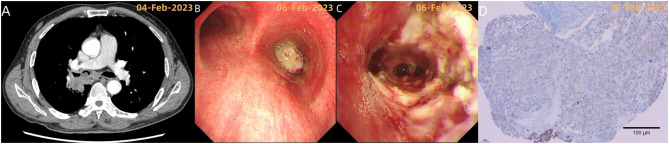
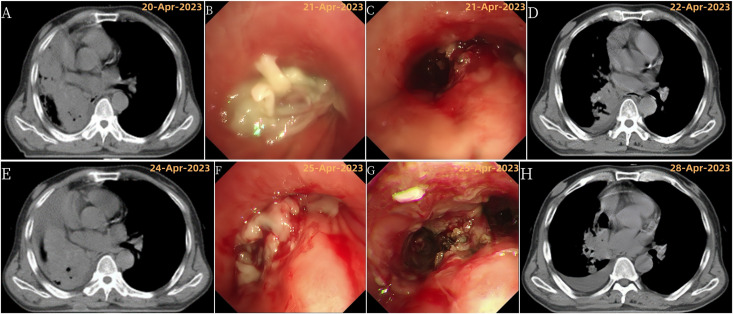
Pulmonary sarcomatoid carcinoma (PSC), a rare non-small cell lung cancer (NSCLC) subtype, poses diagnostic and treatment difficulties. Current research explores targeted therapies and immunotherapy to improve patient outcomes. This case report details a male patient diagnosed with PSC via pathology. Tests revealed high levels of PD-L1, a marker suggesting potential benefit from immune checkpoint inhibitors. However, despite bronchoscopic intervention, his advanced stage IIIB cancer (cT3N2bM0) progressed quickly, with progression-free survival (PFS) under 3 months. Following progression, the patient received tislelizumab (anti-PD-1 antibody) and anlotinib (an anti-angiogenic drug) as second-line therapy. This combination showed promise, achieving near-partial remission after the first cycle. Subsequent scans documented continued tumor shrinkage until the patient experienced fatal hemoptysis. This case highlights the potential benefits of combining tislelizumab with anlotinib for PSC. However, it also represents the first reported case of fatal hemoptysis with this specific treatment regimen. This finding emphasizes the need for increased awareness of this potential complication, especially in patients with centrally located PSC treated with anti-angiogenic agents like anlotinib.
Keywords: adverse effects; anlotinib; hemoptysis; pulmonary sarcomatoid carcinoma; tislelizumab.
Copyright © 2024 Pu, Ma, Peng and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Manzotti G, Torricelli F, Benedetta D, Lococo F, Sancisi V, Rossi G, et al. An epithelial-to-mesenchymal transcriptional switch triggers evolution of pulmonary sarcomatoid carcinoma (PSC) and identifies dasatinib as new therapeutic option. Clin Cancer Res. (2019) 25:2348–60. doi: 10.1158/1078-0432.CCR-18-2364 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials