

Cryptococcus neoformans osteomyelitis of the radius treatment with antifungal calcium sulphate: A case report and literature review
- PMID: 39403459
- PMCID: PMC11471500
- DOI: 10.1016/j.heliyon.2024.e37514
Cryptococcus neoformans osteomyelitis of the radius treatment with antifungal calcium sulphate: A case report and literature review
Abstract
Background: Cryptococcus neoformans is an opportunistic fungal pathogen widely distributed in nature, commonly found in soil and bird droppings such as pigeons. Cryptococcal osteomyelitis is usually found in immunocompromised patients, in an unusual condition Cryptococcus invades the bone. It usually occurs as a part of disseminated infection and is rarely isolated, and isolated cryptococcal osteomyelitis of the radius is rarer.
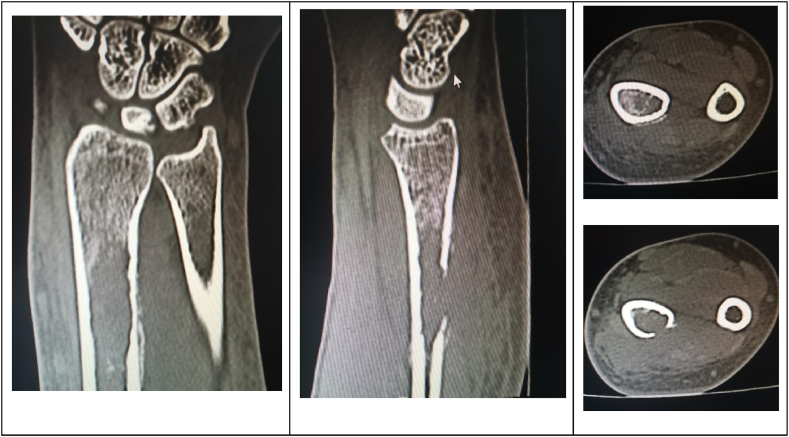
Case presentation: We report a case of a 41-year-old woman with no underlying disease who presented with progressive distal swelling of the left forearm. The patient was initially suspected by local doctors of a malignant bone tumor. For further diagnosis, we performed a computed tomography-guided biopsy of the radius and found granulomatous inflammation with massive macrophage infiltration and a specific stain showing mycosis. Genetic testing revealed a high abundance of Cryptococcus neoformans. We performed debridement of the radius and filled the bone defect with antifungal calcium sulfate. Fluconazole was taken orally for 3 months after operation. No recurrence was found in the 15-month follow-up.
Conclusion: It is the second case of Cryptococcus osteomyelitis as the only manifestation of extrapulmonary disease since 1973. It should be a safe and effective method to eliminate dead space, release antifungal drugs for a long time and increase bone stability by filling bone defect with antifungal drugs and calcium sulfate bone powder.
Keywords: Calcium sulfate; Case report; Cryptococcus; Fungus; Osteomyelitis; Radius.
© 2024 Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that there are no conflicts of interest, financial or other conflicts of interest.
Figures








Similar articles
-
Isolated cryptococcal osteomyelitis of the sacrum in an immunocompetent patient: a case report and literature review.BMC Infect Dis. 2023 Feb 24;23(1):116. doi: 10.1186/s12879-023-08066-6. BMC Infect Dis. 2023. PMID: 36829132 Free PMC article. Review.
-
Cryptococcal osteomyelitis of the Zygomatic bone: a case report.BMC Infect Dis. 2020 Jun 5;20(1):399. doi: 10.1186/s12879-020-05123-2. BMC Infect Dis. 2020. PMID: 32503446 Free PMC article.
-
Isolated cryptococcal osteomyelitis of the ulna in an immunocompetent patient: A case report.World J Clin Cases. 2022 Jul 6;10(19):6617-6625. doi: 10.12998/wjcc.v10.i19.6617. World J Clin Cases. 2022. PMID: 35979300 Free PMC article.
-
Cryptococcus neoformans osteomyelitis of the tibia: a case report and review of the literature.J Med Case Rep. 2023 May 7;17(1):188. doi: 10.1186/s13256-023-03925-x. J Med Case Rep. 2023. PMID: 37149631 Free PMC article. Review.
-
Cryptococcus neoformans osteomyelitis of the calcaneus: Case report and literature review.SAGE Open Med Case Rep. 2021 Jul 17;9:2050313X211027094. doi: 10.1177/2050313X211027094. eCollection 2021. SAGE Open Med Case Rep. 2021. PMID: 34350000 Free PMC article.
References
-
- Ruan Q., Zhu Y., Chen S., Zhu L., Zhang S., Zhang W. Disseminated cryptococcosis with recurrent multiple abscesses in an immunocompetent patient: a case report and literature review. BMC Infect. Dis. 2017 May 30;17(1):369. doi: 10.1186/s12879-017-2459-9. PMID: 28558705; PMCID: PMC5450334. - DOI - PMC - PubMed
Further reading
-
- Korean Society for Chemotherapy; Korean Society of Infectious Diseases. Orthopaedic Association Korean. Clinical guidelines for the antimicrobial treatment of bone and joint infections in Korea. Infect Chemother. 2014 Jun;46(2):125–138. doi: 10.3947/ic.2014.46.2.125. Epub 2014 Jun 20. PMID: 25024877; PMCID: PMC4091374. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
