

Novel Fluorescence-Based Methods to Determine Infarct and Scar Size in Murine Models of Reperfused Myocardial Infarction
- PMID: 39404396
- PMCID: PMC11475149
- DOI: 10.3390/cells13191633
Novel Fluorescence-Based Methods to Determine Infarct and Scar Size in Murine Models of Reperfused Myocardial Infarction
Abstract
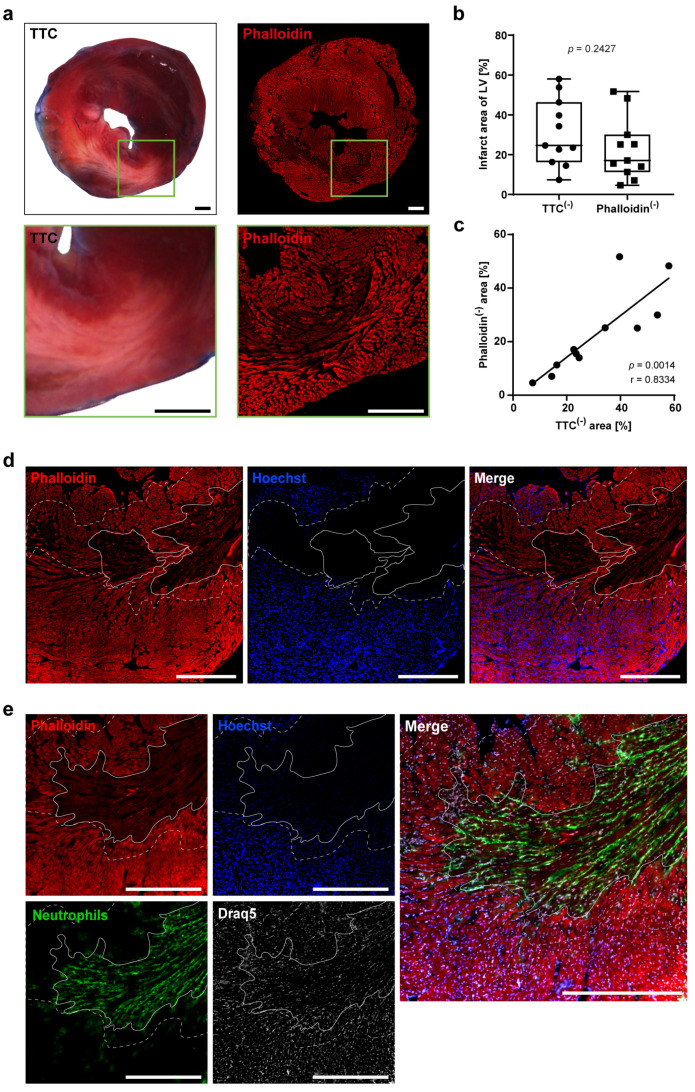
Determination of infarct and scar size following myocardial infarction (MI) is commonly used to evaluate the efficacy of potential cardioprotective treatments in animal models. However, histological methods to determine morphological features in the infarcted heart have barely improved since implementation while still consuming large parts of the tissue and offering little options for parallel analyses. We aim to develop a new fluorescence technology for determining infarct area and area at risk that is comparable to 2,3,5-triphenyltetrazolium chloride (TTC) staining but allows for multiple analyses on the same heart tissue. For early and late time points following MI, we compared classical histochemical approaches with fluorescence staining methods. Reperfused MI was induced in male mice, the hearts were extracted 24 h, 7-, 21-, or 28-days later and fluorescently stained by combining Hoechst and phalloidin. This approach allowed for clear visualization of the infarct area, the area at ischemic risk and the remote area not affected by MI. The combined fluorescence staining correlated with the classic TTC/Evans Blue staining 24 h after MI (r = 0.8334). In later phases (>7 d) post-MI, wheat germ agglutinin (WGA) is equally accurate as classical Sirius Red (r = 0.9752), Masson's (r = 0.9920) and Gomori's Trichrome (r = 0.8082) staining for determination of scar size. Additionally, feasibility to co-localize fluorescence-stained immune cells in specific regions of the infarcted myocardium was demonstrated with this protocol. In conclusion, this new procedure for determination of post-MI infarct size is not inferior to classical TTC staining, yet provides substantial benefits, including the option for unbiased software-assisted analysis while sparing ample residual tissue for additional analyses. Overall, this enhances the data quality and reduces the required animal numbers consistent with the 3R concept of animal experimentation.
Keywords: 3R; histology; infarct size; myocardial infarction; scar size.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



References
-
- Roth G.A., Mensah G.A., Johnson C.O., Addolorato G., Ammirati E., Baddour L.M., Barengo N.C., Beaton A.Z., Benjamin E.J., Benziger C.P., et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020;76:2982–3021. doi: 10.1016/j.jacc.2020.11.010. - DOI - PMC - PubMed
-
- Takagawa J., Zhang Y., Wong M.L., Sievers R.E., Kapasi N.K., Wang Y., Yeghiazarians Y., Lee R.J., Grossman W., Springer M.L. Myocardial infarct size measurement in the mouse chronic infarction model: Comparison of area- and length-based approaches. J. Appl. Physiol. 2007;102:2104–2111. doi: 10.1152/japplphysiol.00033.2007. - DOI - PMC - PubMed
-
- Fishbein M.C., Meerbaum S., Rit J., Lando U., Kanmatsuse K., Mercier J.C., Corday E., Ganz W. Early phase acute myocardial infarct size quantification: Validation of the triphenyl tetrazolium chloride tissue enzyme staining technique. Am. Heart J. 1981;101:593–600. doi: 10.1016/0002-8703(81)90226-X. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
