

Conventional one-handed compared to two-handed endoscopic ear surgery using an endoscope holder: a single center study
- PMID: 39404878
- PMCID: PMC11890327
- DOI: 10.1007/s00405-024-09018-9
Conventional one-handed compared to two-handed endoscopic ear surgery using an endoscope holder: a single center study
Abstract
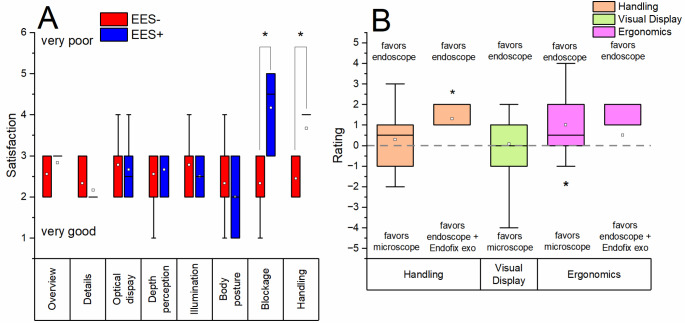
Introduction: One-handedness is a challenge in conventional endoscopic ear surgery (EES). We present results on the first-ever application of the passive endoscope holder 'Endofix exo' (Co. AKTORmed GmbH, Neutraubling, Germany) in EES, which enables two-handed surgery.
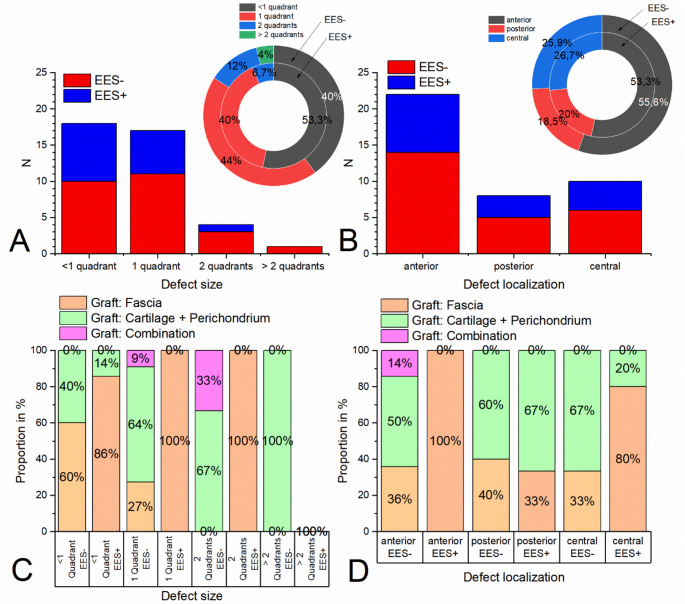
Methods: This two-sided study compares cut-suture time, operating time, postoperative complications, graft take rates, hearing results and quality of life in patients who underwent first stage tympanoplasty due to tympanic membrane perforation with intact ossicular chain conditions. 25 patients received classic EES (EES-, mean age: 28 ± 21 years) and 15 received EES with the passive holder (EES+, mean age: 48 ± 21 years).
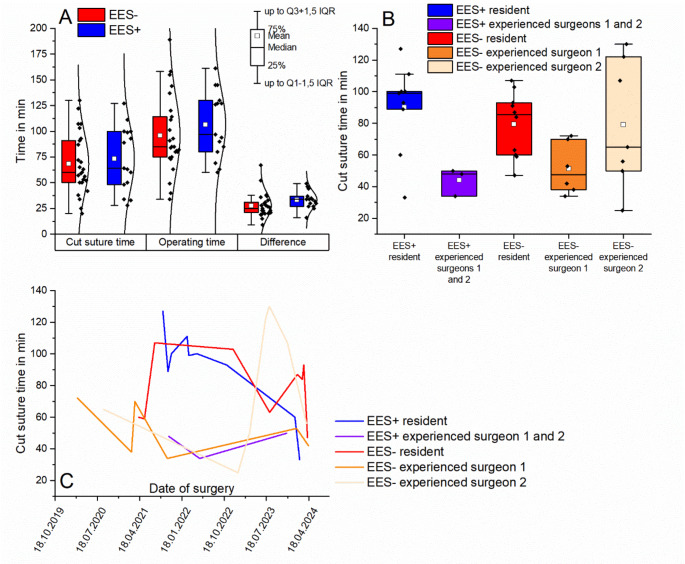
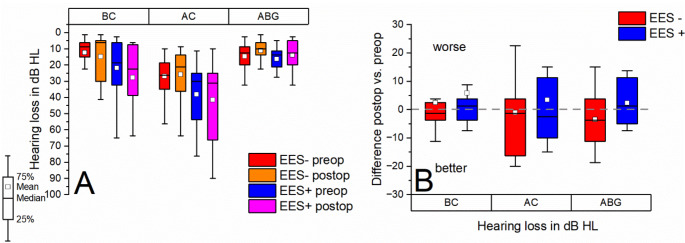
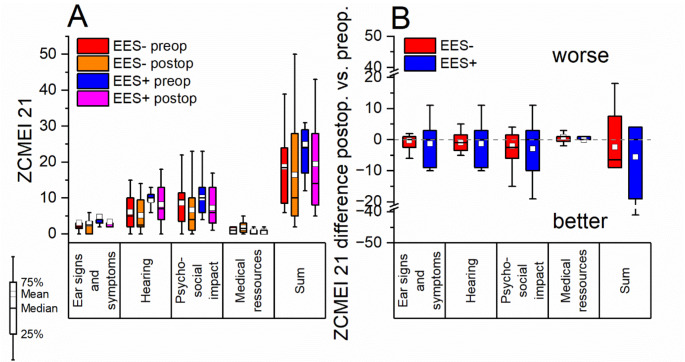
Results: Mean operating times (EES-: 96 ± 38 (SD) min; EES+: 107 ± 33 min), cut-suture times (EES-: 68 ± 30 min; EES+: 73 ± 31 min), complications, graft take rates and hearing results (preoperative air bone gap (ABG) (PTA4): 15 dB ± SD 8 dB (EES-); 16 dB ± SD 8 dB (EES+); postoperative ABG (PTA4): 11.25dB ± SD 11.3dB (EES-); 14 dB ± SD 10 dB (EES+)) did not differ significantly (p > 0.05) between the two groups. Postoperative hearing results and quality of life tended to improve in both groups (p > 0.05).
Discussion: The passive endoscope holder has been successfully applied during the course of the study. However, modifications of the endoscope holder and further studies are recommended focusing on positioning of grafts and prostheses to obtain conclusive results regarding the superiority of two-handed EES over one-handed conventional EES.
Keywords: Cut-suture time; Passive endoscope holder; Postoperative outcome; Surgical assistance system; Two-handed endoscopic ear surgery.
© 2024. The Author(s).
Conflict of interest statement
Financial disclosures/conflicts of interest: There are no financial disclosures or conflicts of interest. Approval of local ethics committee: The study followed the review and approval of the local ethics committee at the Technische Universität Dresden (BO-EK-4012022). Disclosure of potential conflicts of interest: The authors disclose that no conflicts of interest (financial or nonfinancial) occurred in the course of the study and the preparation of this paper. Research involving human participants/informed consent: The study was conducted in accordance with the Declaration of Helsinki and according to the rules of good clinical practice, following the review and approval of the local ethics committee at the Technische Universität Dresden (BO-EK-4012022).
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
