

A More Efficient and Safer Improved Percutaneous Pedicle Screw Insertion Technique-Trajectory Dynamic Adjustment Technique, Technical Note, and Clinical Efficacy
- PMID: 39406475
- PMCID: PMC11735363
- DOI: 10.1111/os.14260
A More Efficient and Safer Improved Percutaneous Pedicle Screw Insertion Technique-Trajectory Dynamic Adjustment Technique, Technical Note, and Clinical Efficacy
Abstract
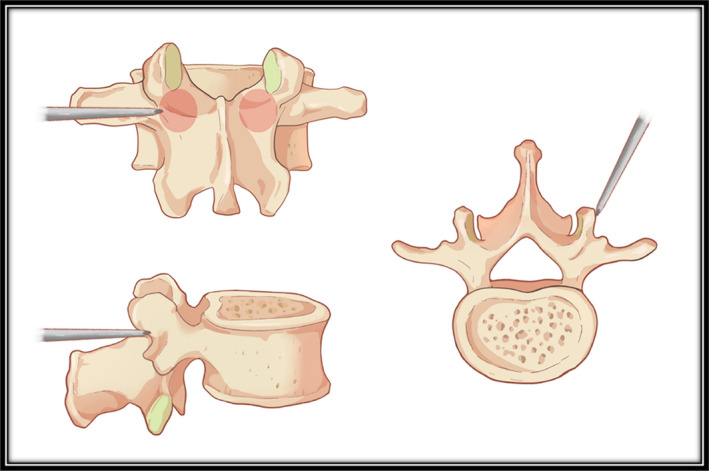
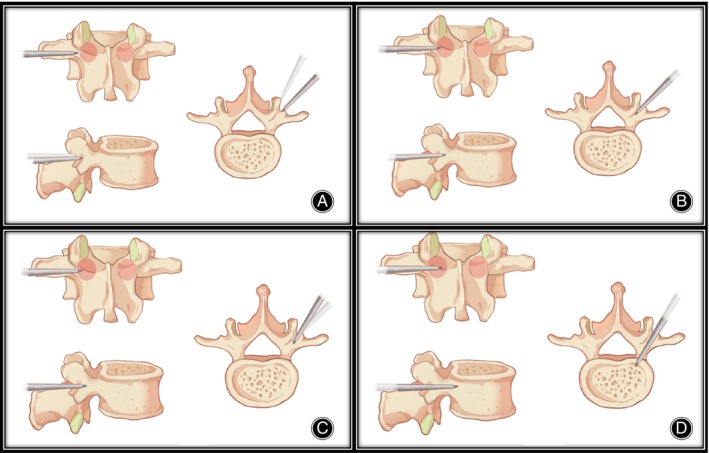
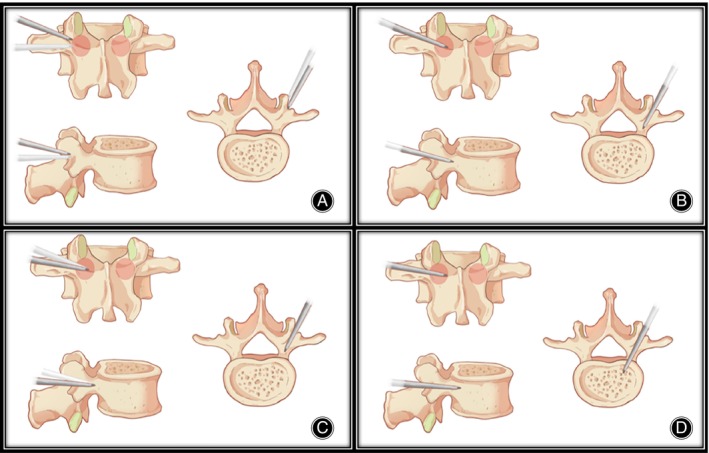
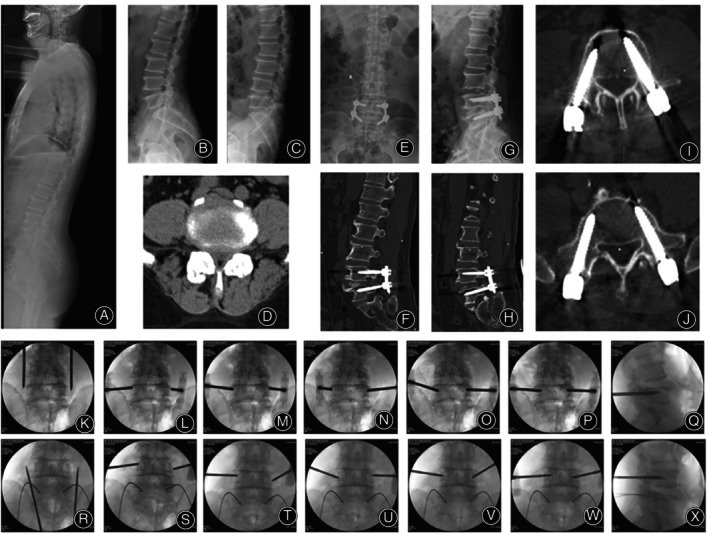
Objective: Percutaneous pedicle screw fixation (PPSF) technique requires a very precise entry point of the Jamshidi needle, which leads to repeated adjustments, damaging the pedicle and increasing radiation exposure. This study was designed to propose an improved percutaneous pedicle screw fixation technique-trajectory dynamic adjustment (TDA) technique, and evaluate its feasibility and assess the clinical outcomes.
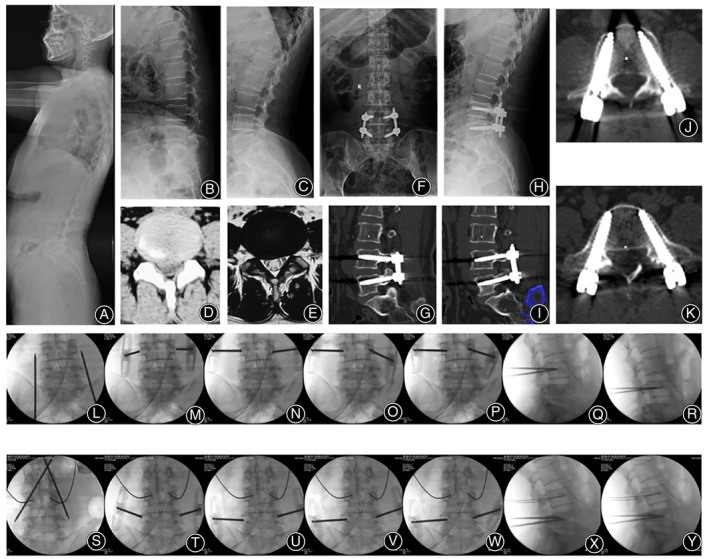
Method: A total of 445 patients with lumbar spondylolisthesis or lumbar spinal stenosis associated with instability from June 2017 to May 2022 were included in the retrospective study. They were randomly separated into two groups. Two hundred thirty-one patients underwent TDA technique (TDA group). Two hundred fourteen patients underwent traditional PPSF technique (PPSF group). All patients underwent postoperative CT to assess the accuracy of screw placement, superior facet joint violation (FJV). The evaluated clinical outcomes were needle insertion time, radiation exposure, blood loss, hospital stay, the Japanese Orthopedic Association (JOA) score, the Visual Analogue Scale (VAS) scores for lower back pain (LBP), and leg pain, lumbar interbody fusion rate, and postoperative complications. The independent-sample t test and paired t-test were used for continuous data. The contingency table and Mann-Whitney U test were used for categorical data.
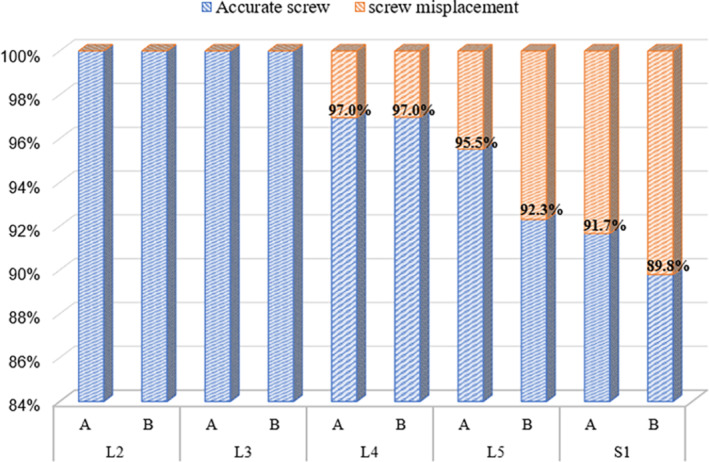
Results: The time of the insertion in TDA group was significantly lower than that in PPSF group (p < 0.05). Similarly, the fluoroscopy frequency in TDA group was significantly lower than that in PPSF group (p < 0.05). There was no difference in intraoperative blood loss and hospital stay between the two groups (p > 0.05). Overall, there was no significant difference in the proportion of clinically acceptable screws between the two groups (p > 0.05). In addition, the lateral screw misplacement in TDA group was higher. Moreover, FJV rate was significantly lower than that in PPSF group (p < 0.05). In both TDA group and PPSF group, postoperative back and leg pain and the JOA score were significantly improved (p < 0.05). However, there were no significant differences in the pre- and postoperative VAS score for back and leg pain and the JOA score, JOA recovery rate, intervertebral fusion rate, and complications rate between the two groups (p > 0.05).
Conclusion: Compared to traditional PPSF technique, TDA technique is a safer and more effective procedure which has shorter surgical time, lower radiation exposure, and lower facet joint violation rate.
Keywords: facet joint violation; lumbar; minimally invasive; percutaneous pedicle screw fixation; radiation exposure.
© 2024 The Author(s). Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Magerl F., “External Skeletal Fixation of the Lower Thoracic and the Lumbar Spine,” in Current Concepts of External Fixation of Fractures, eds. Uhthoff H. K. and Stahl E. (Berlin, Heidelberg: Springer Berlin Heidelberg, 1982), 353–366.
-
- Anand N., Baron E. M., Thaiyananthan G., Khalsa K., and Goldstein T. B., “Minimally Invasive Multilevel Percutaneous Correction and Fusion for Adult Lumbar Degenerative Scoliosis: A Technique and Feasibility Study,” Journal of Spinal Disorders & Techniques 21 (2008): 459–467, 10.1097/BSD.0b013e318167b06b. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
