

Immunotherapy for glioblastoma: current state, challenges, and future perspectives
- PMID: 39406966
- PMCID: PMC11607068
- DOI: 10.1038/s41423-024-01226-x
Immunotherapy for glioblastoma: current state, challenges, and future perspectives
Abstract
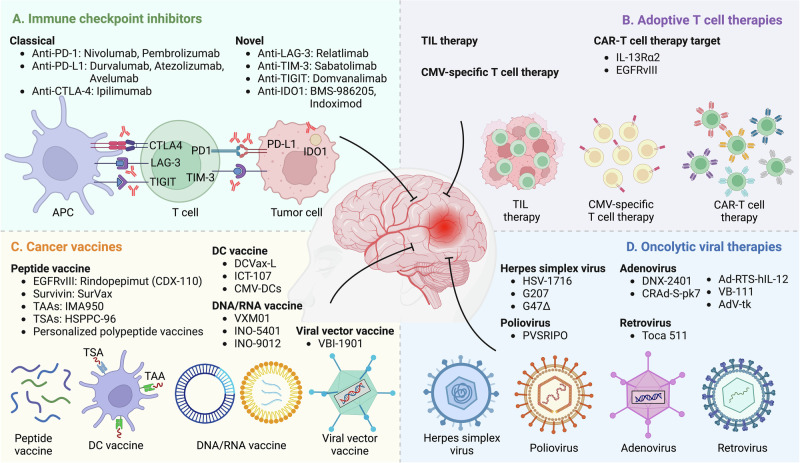
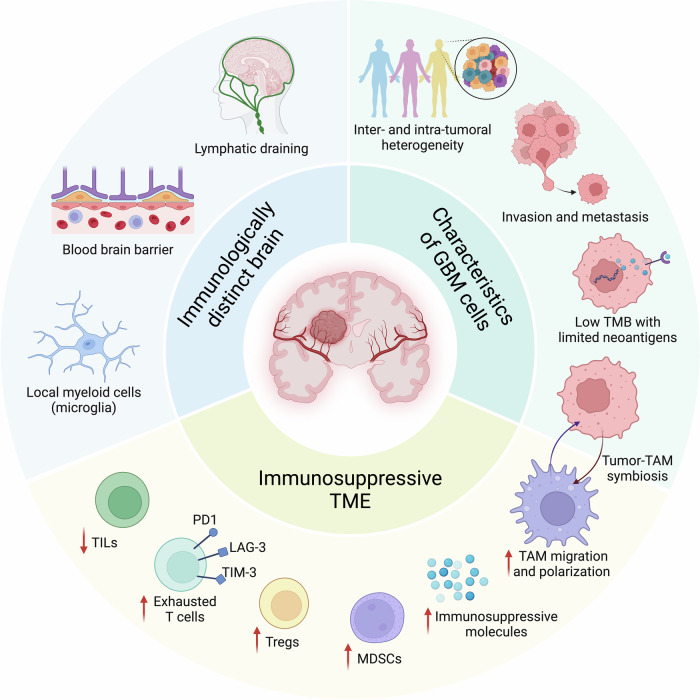
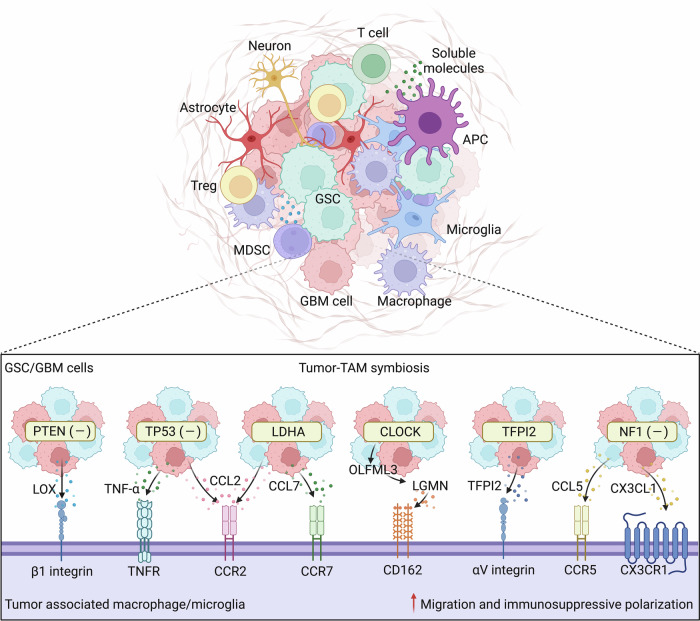
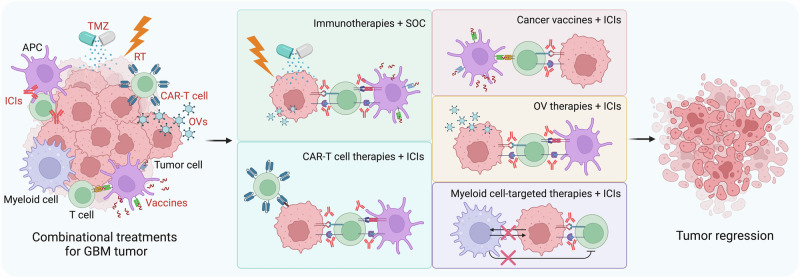
Glioblastoma (GBM) is an aggressive and lethal type of brain tumor in human adults. The standard of care offers minimal clinical benefit, and most GBM patients experience tumor recurrence after treatment. In recent years, significant advancements have been made in the development of novel immunotherapies or other therapeutic strategies that can overcome immunotherapy resistance in many advanced cancers. However, the benefit of immune-based treatments in GBM is limited because of the unique brain immune profiles, GBM cell heterogeneity, and immunosuppressive tumor microenvironment. In this review, we present a detailed overview of current immunotherapeutic strategies and discuss the challenges and potential molecular mechanisms underlying immunotherapy resistance in GBM. Furthermore, we provide an in-depth discussion regarding the strategies that can overcome immunotherapy resistance in GBM, which will likely require combination therapies.
Keywords: Adoptive T-cell therapies; Glioblastoma; Immune checkpoint inhibitors (ICIs); Immunotherapy combination; Oncolytic viral therapies; Tumor vaccines.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: JDL reports being named a coinventor on pending and issued patents held by the Cleveland Clinic relating to cancer therapies, but these are not directly relevant to this review. No potential conflicts of interest are disclosed by the other authors.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
