

Hypothermia versus normothermia in patients with cardiac arrest and shockable rhythm: a secondary analysis of the TTM-2 study
- PMID: 39407230
- PMCID: PMC11481803
- DOI: 10.1186/s13054-024-05119-3
Hypothermia versus normothermia in patients with cardiac arrest and shockable rhythm: a secondary analysis of the TTM-2 study
Abstract
Background: The aim of this study was to assess whether hypothermia increased survival and improved functional outcome when compared with normothermia in out-of-hospital cardiac arrest (OHCA) patients with similar characteristics than in previous randomized studies showing benefits for hypothermia.
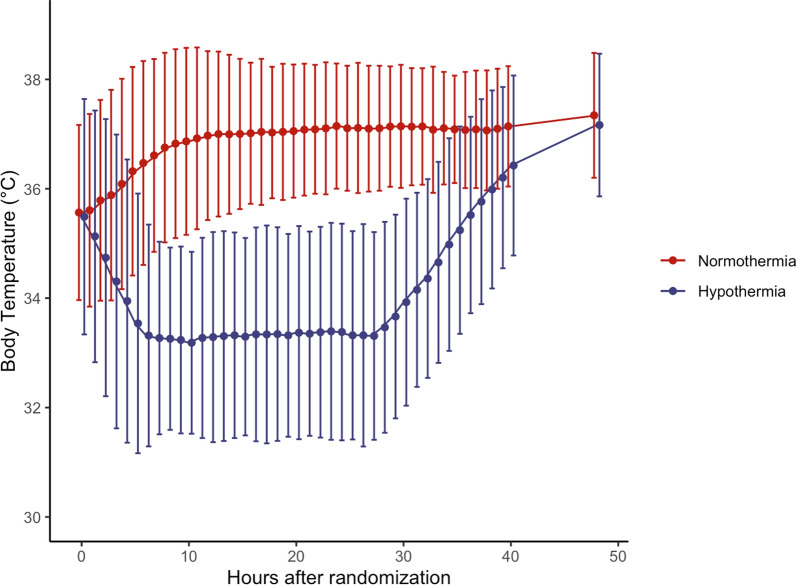
Methods: Post hoc analysis of a pragmatic, multicenter, randomized clinical trial (TTM-2, NCT02908308). In this analysis, the subset of patients included in the trial who had similar characteristics to patients included in one previous randomized trial and randomized to hypothermia at 33 °C or normothermia (i.e. target < 37.8 °C) were considered. The primary outcome was survival at 6 months; secondary outcomes included favorable functional outcome at 6 months, defined as a modified Rankin scale of 0-3. Time-to-death and the occurrence of adverse events were also reported.
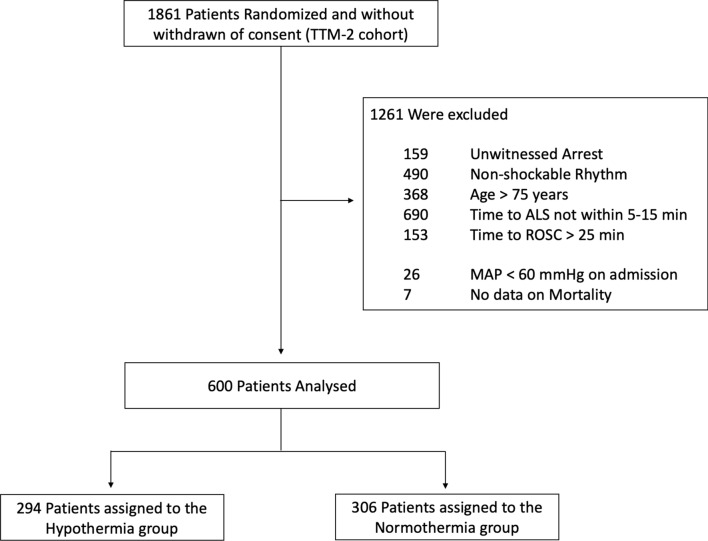
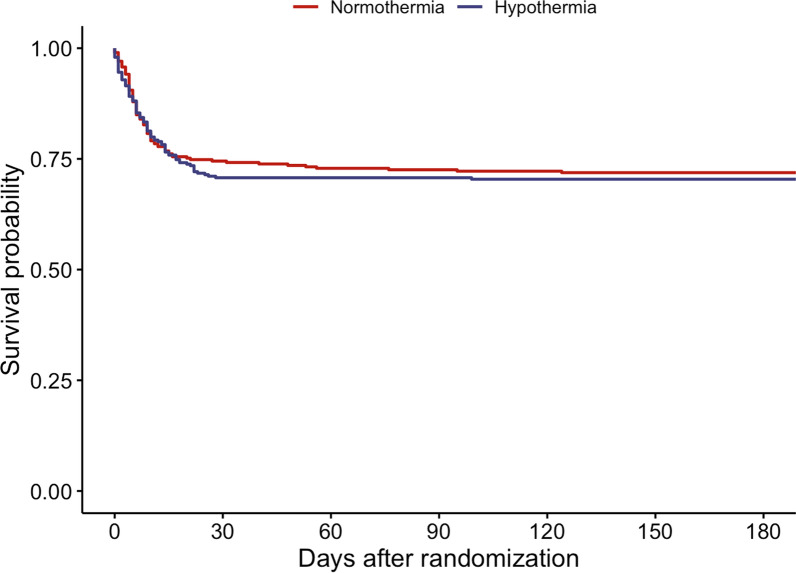
Results: From a total of 1891 included in the TTM-2 study, 600 (31.7%) were included in the analysis, 294 in the hypothermia and 306 in the normothermia group. At 6 months, 207 of the 294 patients (70.4%) in the hypothermia group and 220 of the 306 patients (71.8%) in the normothermia group had survived (relative risk with hypothermia, 0.96; 95% confidence interval [CI], 0.81 to 1.15; P = 0.71). Also, 198 of the 294 (67.3%) in the hypothermia group and 202 of the 306 (66.0%) in the normothermia group had a favorable functional outcome (relative risk with hypothermia, 1.03; 95% CI, 0.87 to 1.23; P = 0.79). There was a significant increase in the occurrence of arrythmias in the hypothermia group (62/294, 21.2%) when compared to the normothermia group (43/306, 14.1%-OR 1.49, 95% CI 1.05-2.14; p = 0.026).
Conclusions: In this study, hypothermia at 33˚C did not improve survival or functional outcome in a subset of patients with similar cardiac arrest characteristics to patients in whom benefit from hypothermia was shown in prior studies.
Keywords: Cardiac arrest; Hypothermia; Outcome; Shockable rhythm.
© 2024. The Author(s).
Conflict of interest statement
A Cariou, P Young, and T R Keeble reported receiving lecture fees from BD. FS Taccone received lecture fees from BD and ZOLL and is scientific advisor for Nihon Khoden, Neuroptics and Eurosets. C Robba received lectures fees from Integra, BD and Edwards. N Nielsen received lecture fees from Bard Medical and consulting fees from BrainCool. Other authors reported no potential conflict of interest relevant to this study.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
