

Relationship between Preoperative Red Cell Distribution Width and Prolonged Postoperative Use of Catecholamines in Minimally Invasive Mitral Valve Surgery Patients: A Retrospective Cohort Study
- PMID: 39407797
- PMCID: PMC11476661
- DOI: 10.3390/jcm13195736
Relationship between Preoperative Red Cell Distribution Width and Prolonged Postoperative Use of Catecholamines in Minimally Invasive Mitral Valve Surgery Patients: A Retrospective Cohort Study
Abstract
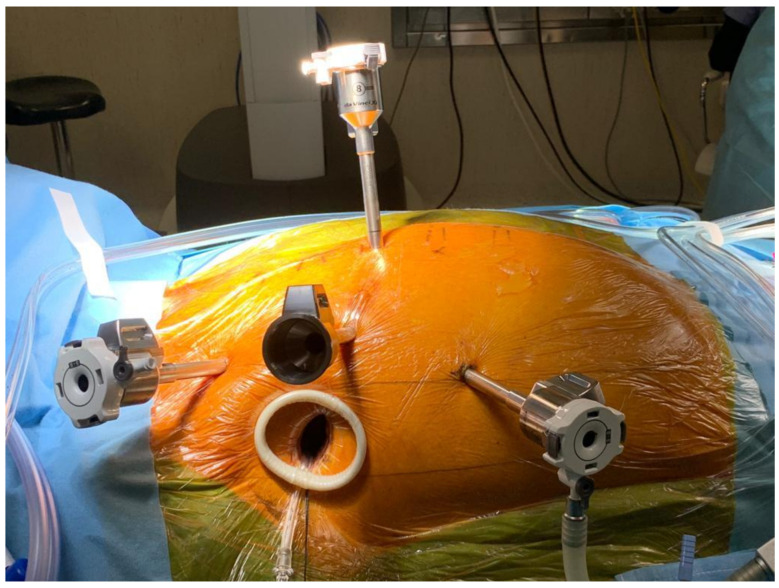
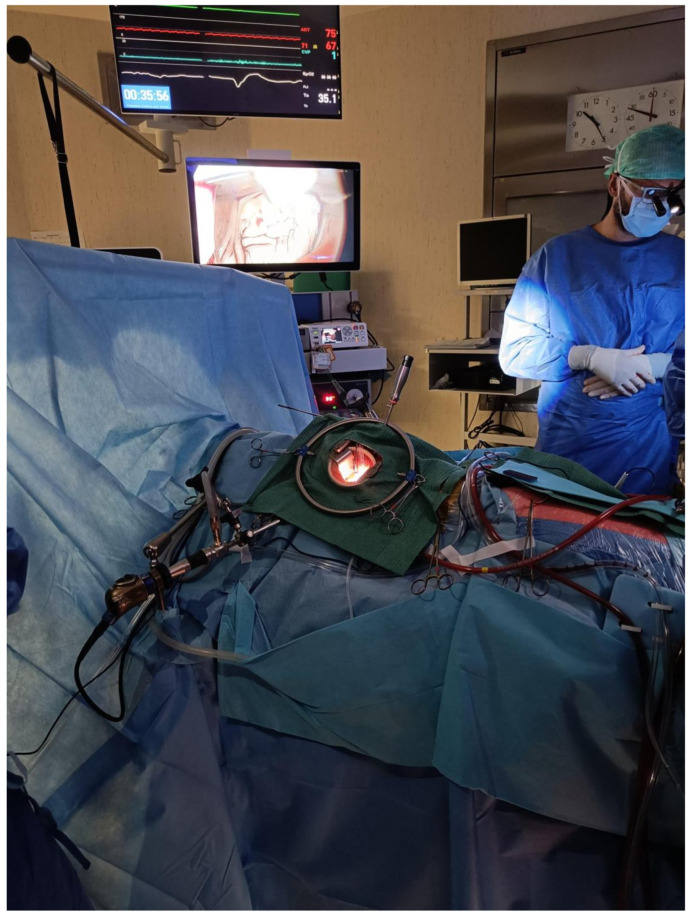
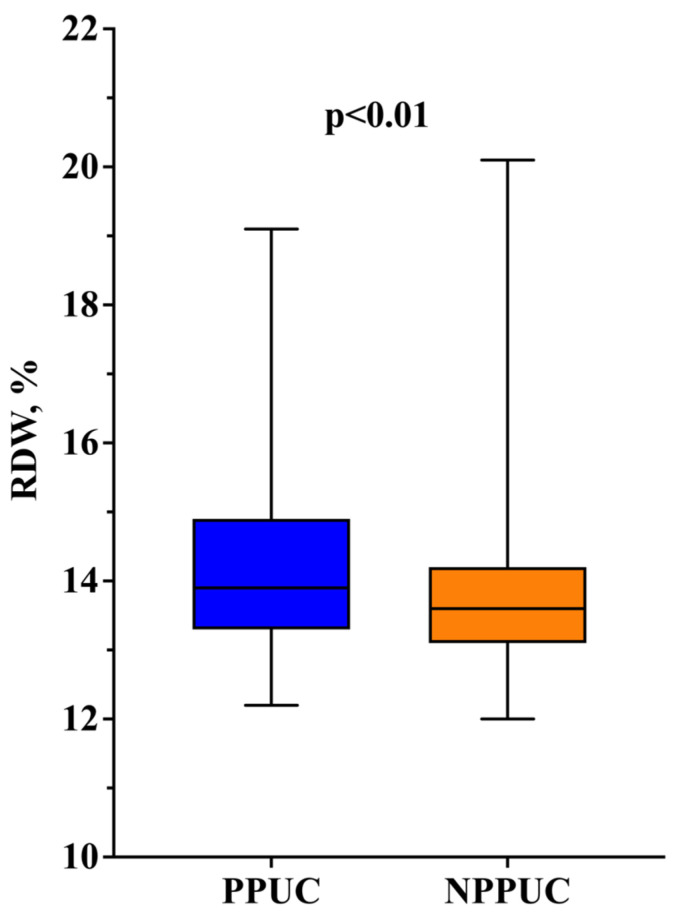
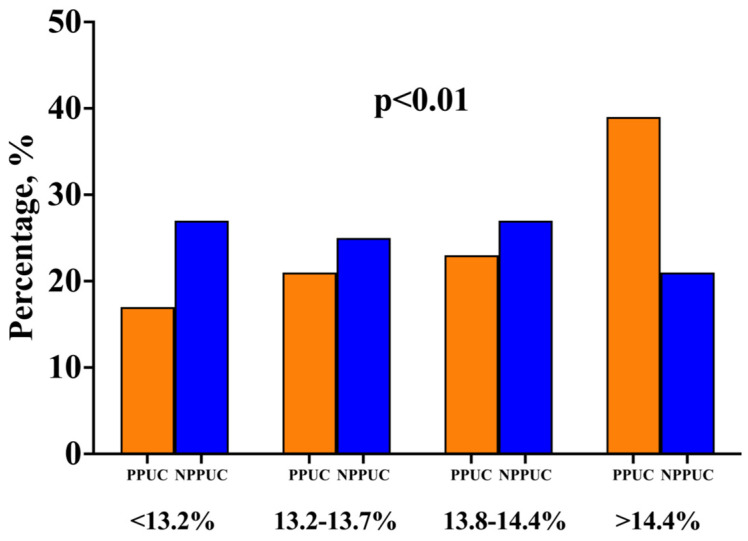
Background/Objectives: Elevated RDW has emerged in cardiac surgery as a potential means of preoperative risk stratification with the capacity to predict short- and long-term postoperative mortality, acute kidney injury, and postoperative atrial fibrillation. The question as to whether perioperative hemodynamic instability may be predicted by such a marker remains a topic of ongoing debate. The aim of this study was to explore the relationship between preoperative RDW and prolonged postoperative catecholamine use in minimally invasive mitral valve surgery. Methods: We performed a retrospective monocentric cohort study in an academic hospital; we enrolled patients who had undergone minimally invasive mitral valve surgery (including both robot-assisted and non-robot-assisted procedures) between January 2019 and December 2022. We considered the use of inotropes and/or vasopressors for at least twelve hours after post-surgery ICU admission to qualify as the prolonged postoperative use of catecholamines (PPUC). The RDW was obtained from the routine full blood count analysis performed upon admission or a maximum of 72 h before surgery. We also performed a multivariable logistic regression analysis with PPUC as the dependent variable. Results: We finally enrolled 343 patients. Upon multivariate analysis, RDW >14.4% was independently associated with prolonged postoperative catecholamine use when compared to the reference group (OR 2.62 [1.06-4.84]; p = 0.03). Moreover, the EuroSCORE II score (OR 1.38 [1.03-1.85]; p = 0.03), the cross-clamp time (OR 1.01 [1.01-1.02]; p < 0.01), and robot-assisted mitral valve surgery (OR 0.53 [0.30-0.93]; p < 0.03) were independently associated with the prolonged postoperative use of catecholamines. Conclusions: This study identified that an elevated preoperative RDW (>14.4%), the EuroSCORE II score, and the cross-clamp time independently predict prolonged postoperative catecholamine use in minimally invasive mitral valve surgery patients. Conversely, the robot-assisted approach was associated with a smaller hemodynamic impairment.
Keywords: RDW; cardiac surgery; robotic surgery.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Risk Factors for Higher Postoperative Myocardial Injury in Minimally Invasive Mitral Valve Surgery Patients: A Cohort Study.J Clin Med. 2024 Mar 10;13(6):1591. doi: 10.3390/jcm13061591. J Clin Med. 2024. PMID: 38541817 Free PMC article.
-
Early Postoperative Complications of Robotic-assisted Versus Minimally Invasive Mitral Valve Surgery: A Propensity Score-matched Analysis.J Cardiothorac Vasc Anesth. 2024 Sep;38(9):1996-2001. doi: 10.1053/j.jvca.2024.05.026. Epub 2024 May 23. J Cardiothorac Vasc Anesth. 2024. PMID: 38942684
-
Aortic cross-clamp time correlates with mortality in the mini-mitral international registry.Eur J Cardiothorac Surg. 2023 Jun 1;63(6):ezad147. doi: 10.1093/ejcts/ezad147. Eur J Cardiothorac Surg. 2023. PMID: 37052525
-
Minithoracotomy versus sternotomy in mitral valve surgery: meta-analysis from recent matched and randomized studies.J Cardiothorac Surg. 2023 Apr 6;18(1):101. doi: 10.1186/s13019-023-02229-x. J Cardiothorac Surg. 2023. PMID: 37024952 Free PMC article. Review.
-
Is robotic assistance an added value in minimally invasive mitral valve surgery? A meta-analysis from propensity score-matched series.Asian Cardiovasc Thorac Ann. 2023 May;31(4):369-377. doi: 10.1177/02184923231166352. Epub 2023 Mar 29. Asian Cardiovasc Thorac Ann. 2023. PMID: 36987688 Review.
Cited by
-
Risk Factors for Postoperative Acute Kidney Injury Requiring Renal Replacement Therapy in Patients Undergoing Heart Valve Surgery.J Clin Med. 2024 Dec 20;13(24):7811. doi: 10.3390/jcm13247811. J Clin Med. 2024. PMID: 39768734 Free PMC article.
-
Usefulness of Myocardial Injury Parameters in Predicting Prolonged Postoperative Use of Inotropes Drugs in Patients Undergoing Heart Valve Surgery.J Clin Med. 2025 Apr 15;14(8):2719. doi: 10.3390/jcm14082719. J Clin Med. 2025. PMID: 40283552 Free PMC article.
References
-
- Dixon B., Santamaria J.D., Reid D., Collins M., Rechnitzer T., Newcomb A.E., Nixon I., Yii M., Rosalion A., Campbell D.J. The association of blood transfusion with mortality after cardiac surgery: Cause or confounding? (CME) Transfusion. 2013;53:19–27. doi: 10.1111/j.1537-2995.2012.03697.x. - DOI - PubMed
-
- Argenziano M., Chen J.M., Choudhri A.F., Cullinane S., Garfein E., Weinberg A.D., Smith C.R., Jr., Rose E.A., Landry D.W., Oz M.C. Management of vasodilatory shock after cardiac surgery: Identification of predisposing factors and use of a novel pressor agent. J. Thorac. Cardiovasc. Surg. 1998;116:973–980. doi: 10.1016/S0022-5223(98)70049-2. - DOI - PubMed
-
- Sun X., Zhang L., Hill P.C., Lowery R., Lee A.T., Molyneaux R.E., Corso P.J., Boyce S.W. Is incidence of postoperative vasoplegic syndrome different between off-pump and on-pump coronary artery bypass grafting surgery? Eur. J. Cardiothorac. Surg. 2008;34:820–825. doi: 10.1016/j.ejcts.2008.07.012. - DOI - PubMed
LinkOut - more resources
Full Text Sources
