

NT-proBNP Reflects Left Ventricular Hypertrophy Rather than Left Ventricular Dilatation or Systolic Dysfunction in Patients with Fabry Disease
- PMID: 39408013
- PMCID: PMC11478308
- DOI: 10.3390/jcm13195953
NT-proBNP Reflects Left Ventricular Hypertrophy Rather than Left Ventricular Dilatation or Systolic Dysfunction in Patients with Fabry Disease
Abstract
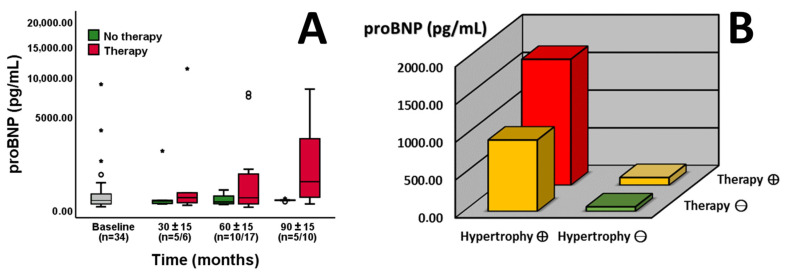
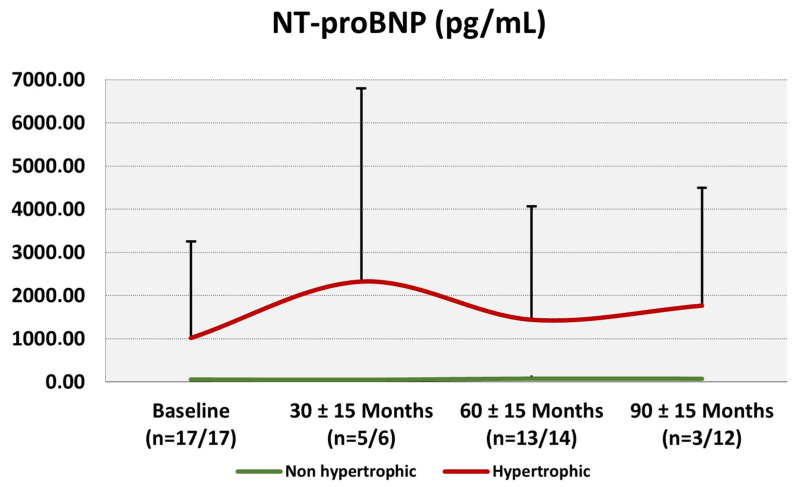
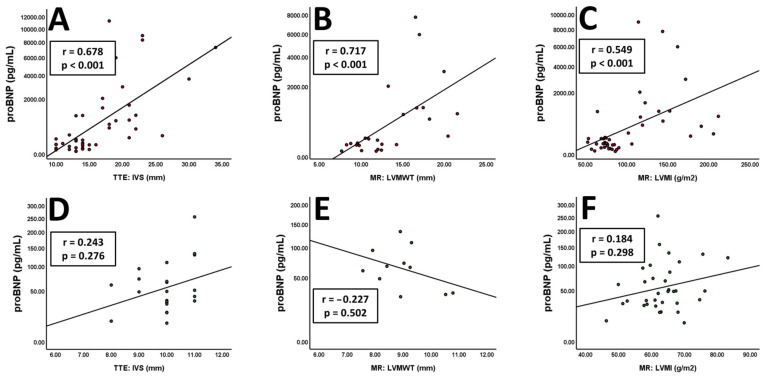
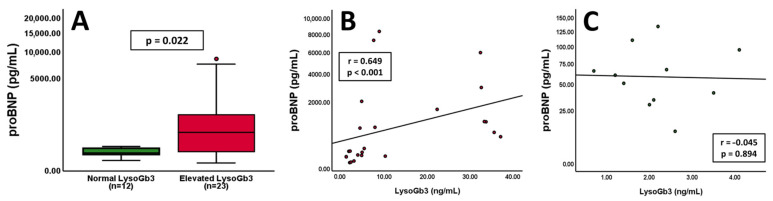
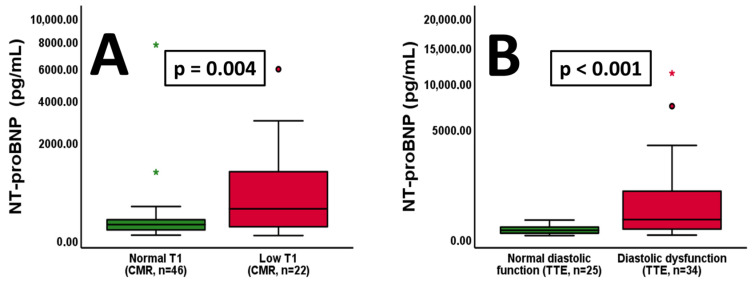
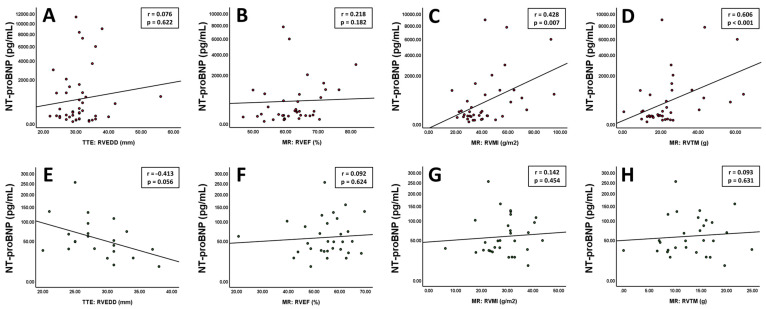
Background: The diagnosis and follow-up of cardiac involvement in Fabry disease constitutes an important challenge for clinicians caring for affected patients. Combining cardiac imaging with laboratory biomarkers appears most appropriate for longitudinal monitoring. Therefore, we examined the use of NT-proBNP and its association with imaging findings in patients with Fabry disease. Methods: We analysed cardiac MRI and echocardiography data, as well as laboratory results, from a single-centre prospective registry. Results: Repetitive follow-ups of 38 patients with Fabry disease, of whom 18 presented with left ventricular hypertrophy (LVH), revealed a correlation of NT-proBNP with left ventricular (LV) interventricular septal thickness, LV maximum wall thickness, LV and right ventricular (RV) mass index and trabecular mass in patients with LVH. Patients without LVH did not exhibit any tangible association between NT-proBNP and the mentioned parameters. Conversely, we could not detect an association of NT-proBNP with impairment of LV or RV ejection fraction or diastolic volume. Conclusions: NT-proBNP plays a pivotal role as a biomarker for cardiac involvement in patients with Fabry disease. Interestingly, in this specific population with mostly preserved ejection fraction, it seems to reflect ventricular hypertrophy rather than ventricular dysfunction or dilatation. While strong associations were found in hypertrophic patients, NT-proBNP's prognostic value appears limited in non- or pre-hypertrophic stages.
Keywords: Fabry disease; NT-proBNP; biomarker; cardiac MRI; cardiomyopathy; echocardiography; lysosomal storage disease.
Conflict of interest statement
C.G. and S.G. received research and congress funding and speaker honoraria from Amicus Therapeutics, Sanofi and Takeda Pharmaceuticals. D.B. received speaker honoraria from Siemens Healthineers. M.P. has received speaker or consulting honoraria from Amicus and participated in meetings sponsored by and received travel funding from Amicus and Sanofi-Genzyme. G.S.-P. received honoraria and research funding from Amicus, Chiesi, Freeline and Sanofi-Genzyme.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
