

Double Row Hip Abductor Reconstruction with Fasciae Latae Transfer for Severe Trendelenburg after Hip Arthroplasty
- PMID: 39408024
- PMCID: PMC11477932
- DOI: 10.3390/jcm13195964
Double Row Hip Abductor Reconstruction with Fasciae Latae Transfer for Severe Trendelenburg after Hip Arthroplasty
Abstract
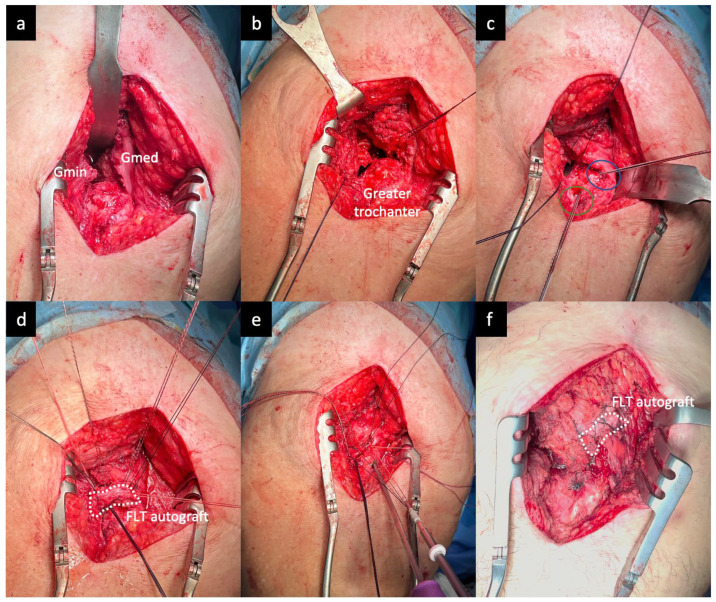
Background/Objectives: Tendinopathy of the gluteus medius and minimus tendons is a primary source of lateral hip pain, ranging from interstitial and partial-thickness tears to complete tears. Treatments include muscle transfers, Achilles tendon allograft procedures, and primary repairs with allografts. This study evaluated the one-year outcomes of gluteus medius and minimus reconstruction using an open double-row technique with a partial tensor fasciae latae transfer for severe Trendelenburg post-total hip arthroplasty. Methods: A prospective study involving eight patients who underwent surgery from April to December 2023 was conducted. The surgery involved an open technique with double-row suture reinforcement and tensor fasciae latae autograft. Outcomes were measured using strength, the Harris Hip Score (HHS), 12-Item Short Form Health Survey (SF-12), Hip Outcome Tool (HOT), International Hip Outcome Tool (iHOT), and Visual Analog Scale (VAS). Follow-ups occurred at 1, 3, 6, 9, and 12 months postoperatively. Results: At an average follow-up of 7.17 months, significant improvements in both hip function and quality of life were observed. The SF-12 quality of life score increased from 27 preoperatively to 34 by month 12. Hip functionality, as measured by the HHS, showed a marked improvement from 48 to 94 points, particularly after six months. The HOT score for hip functionality rose by 23 points by the third month, reaching an average of 86 points. Similarly, the iHOT score increased from 20 to 83 points starting at month 3, reflecting substantial improvements in hip function. Statistically significant improvements were noted at as early as month 3 (p = 0.02), with highly significant gains by month 6 (p < 0.01), which remained stable through month 12 (p < 0.01). Conclusions: Reconstruction of the gluteus medius and minimus tendons using an open double-row technique with a partial tensor fasciae latae transfer significantly enhances hip function and quality of life. Over an average follow-up period of 7.17 months, patients experienced notable improvements. This technique is an effective option for treating lateral hip pain due to tendinopathy.
Keywords: double-row technique; gluteus medius reconstruction; tendinopathy treatment.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Combined Transfer of the Gluteus Maximus and Tensor Fasciae Latae for Irreparable Gluteus Medius Tear Using Contemporary Techniques: Short-Term Outcomes.JB JS Open Access. 2020 Nov 25;5(4):e20.00085. doi: 10.2106/JBJS.OA.20.00085. eCollection 2020 Oct-Dec. JB JS Open Access. 2020. PMID: 33376925 Free PMC article.
-
[Open repair of gluteus medius and minimus tendons tears with double-row technique : Clinical and radiological results].Orthopade. 2018 Mar;47(3):238-245. doi: 10.1007/s00132-017-3524-1. Orthopade. 2018. PMID: 29327070 German.
-
Endoscopic Tendon Compression Bridge Technique for Repair of Partial-Thickness Gluteus Medius Tears With Concomitant Arthroscopy for Labral Tears: Minimum 2-Year Outcomes With Benchmark Control Group.Am J Sports Med. 2023 Dec;51(14):3764-3771. doi: 10.1177/03635465231204314. Epub 2023 Nov 13. Am J Sports Med. 2023. PMID: 37960846
-
Gluteus Maximus Transfer for Irreparable Hip Abductor Deficiency: A Systematic Review and Meta-Analysis.J Arthroplasty. 2024 Apr;39(4):1117-1124.e1. doi: 10.1016/j.arth.2023.10.036. Epub 2023 Oct 23. J Arthroplasty. 2024. PMID: 37879422
-
Influence of Fatty Infiltration on Hip Abductor Repair Outcomes: A Systematic Review and Meta-analysis.Am J Sports Med. 2022 Jul;50(9):2568-2580. doi: 10.1177/03635465211027911. Epub 2021 Sep 8. Am J Sports Med. 2022. PMID: 34495797
References
-
- Seidman A.J., Taqi M., Varacallo M. Trochanteric Bursitis (Archived) StatPearls Publishing; Treasure Island, FL, USA: 2024. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
