

Association between dietary fiber intake and chronic kidney disease in adults with and without hypertension in the United States: a cross-sectional study of NHANES 2009-2020
- PMID: 39412048
- PMCID: PMC11486002
- DOI: 10.1080/0886022X.2024.2415514
Association between dietary fiber intake and chronic kidney disease in adults with and without hypertension in the United States: a cross-sectional study of NHANES 2009-2020
Abstract
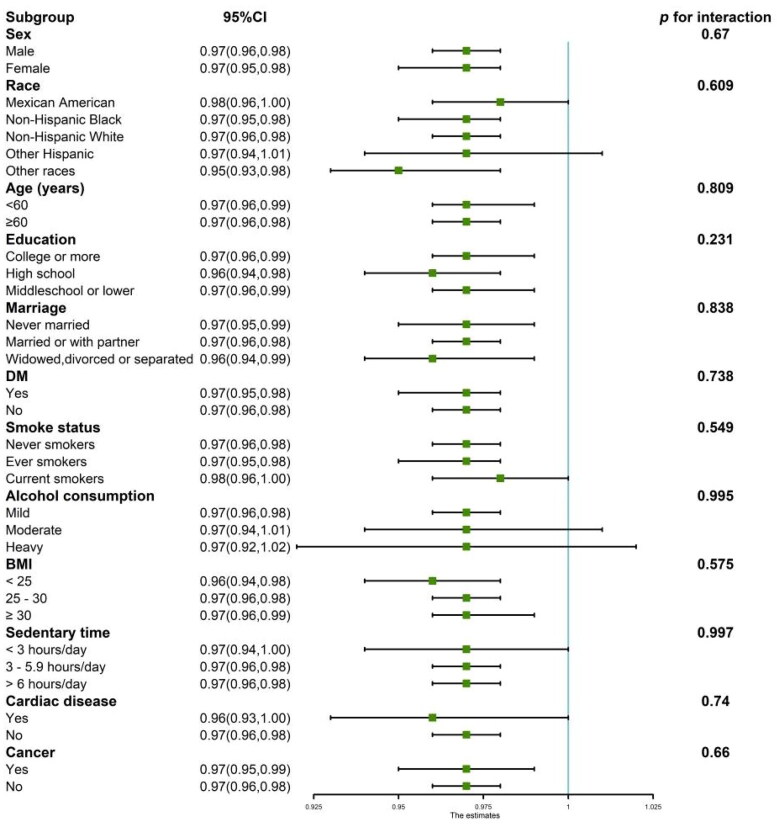
While previous research has highlighted the potential advantages of increasing dietary fiber intake (DFI) for managing hypertension and chronic kidney disease (CKD), there is a gap in large-scale empirical studies examining the relationship between DFI and CKD among hypertensive and nonhypertensive cohorts independently. This study involved 22,871 participants sourced from the NHANES database spanning 2009 to 2020, who were divided into hypertensive (n = 9,861) and nonhypertensive (n = 13,010) groups. The analysis revealed a significant inverse correlation between DFI and CKD prevalence across the sample after adjusting for various covariates (OR = 0.98, 95% CI: 0.97-0.99, p = 0.001). Within the subset of hypertensive individuals, this inverse association mirrors the findings of the overall sample, indicating that a higher DFI was associated with a reduced occurrence of CKD (OR = 0.97, 95% CI: 0.96-0.99, p < 0.001). However, this correlation was not detected in the nonhypertensive group (OR = 0.99, 95% CI: 0.98-1.01, p = 0.285). The RCS analysis further confirmed a pronounced nonlinear inverse relationship between DFI and CKD prevalence in both the entire cohort and the hypertensive group but not in the nonhypertensive group. Further scrutiny of the hypertensive group revealed that individuals with a higher DFI had 33% lower odds of CKD progression for the moderate risk level and 36% lower odds for the high to very high risk level. Subgroup analyses confirmed the consistency of these relationships across various demographics. In summary, this investigation revealed a significant inverse relationship between DFI and CKD prevalence in US adults with hypertension, a relationship not observed in nonhypertensive individuals.
Keywords: Chronic kidney disease; cross-sectional study; dietary fiber intake; hypertension.
Conflict of interest statement
The authors have no competing interests to declare.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous