

Nivolumab+AVD in Advanced-Stage Classic Hodgkin's Lymphoma
- PMID: 39413375
- PMCID: PMC11488644
- DOI: 10.1056/NEJMoa2405888
Nivolumab+AVD in Advanced-Stage Classic Hodgkin's Lymphoma
Abstract
Background: Incorporating brentuximab vedotin into the treatment of advanced-stage classic Hodgkin's lymphoma improves outcomes in adult and pediatric patients. However, brentuximab vedotin increases the toxic effects of treatment in adults, more than half of pediatric patients who receive the drug undergo consolidative radiation, and relapse remains a challenge. Programmed death 1 blockade is effective in Hodgkin's lymphoma, including in preliminary studies involving previously untreated patients.
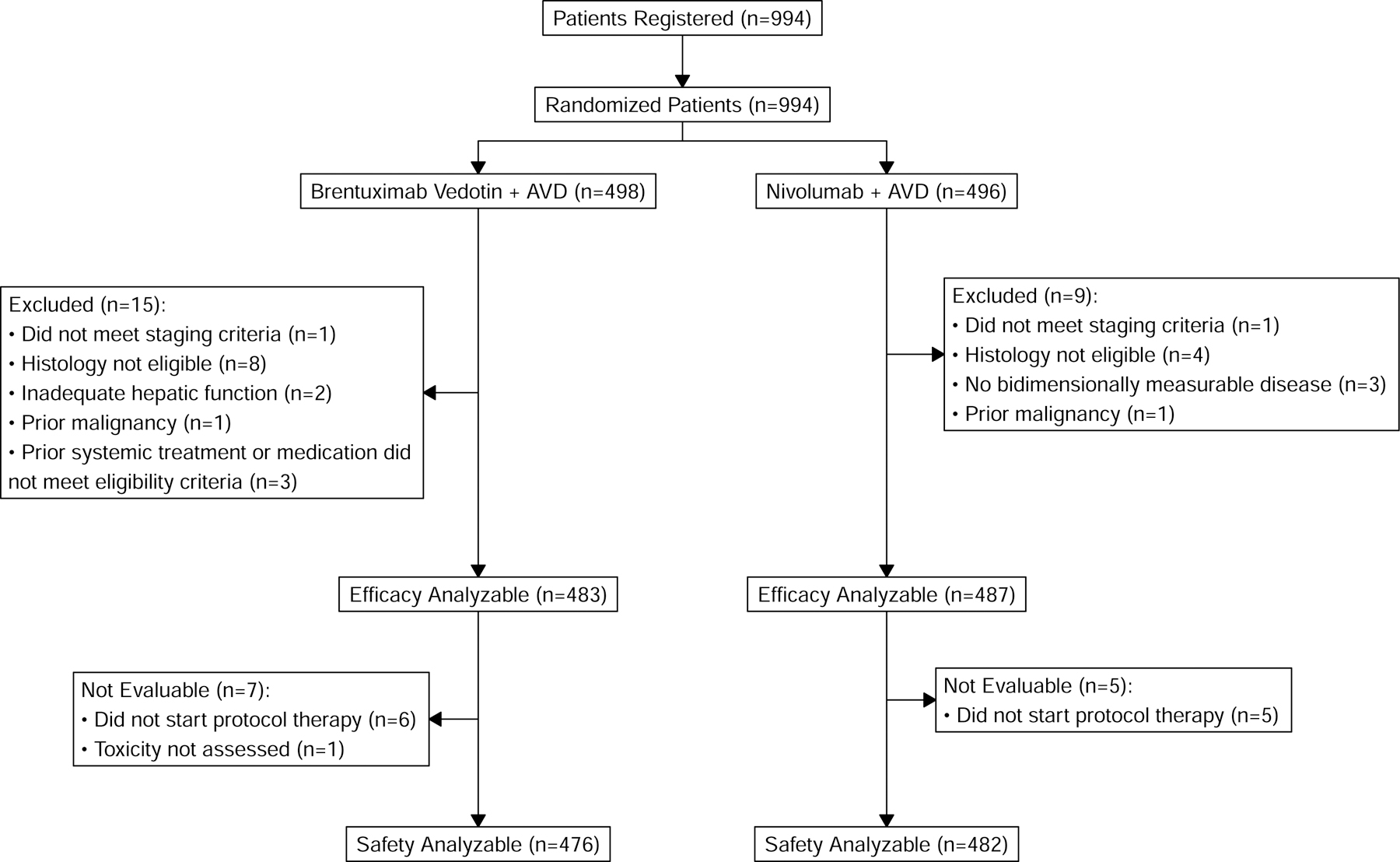
Methods: We conducted a phase 3, multicenter, open-label, randomized trial involving patients at least 12 years of age with stage III or IV newly diagnosed Hodgkin's lymphoma. Patients were randomly assigned to receive brentuximab vedotin with doxorubicin, vinblastine, and dacarbazine (BV+AVD) or nivolumab with doxorubicin, vinblastine, and dacarbazine (N+AVD). Prespecified patients could receive radiation therapy directed to residual metabolically active lesions. The primary end point was progression-free survival, defined as the time from randomization to the first observation of progressive disease or death from any cause.
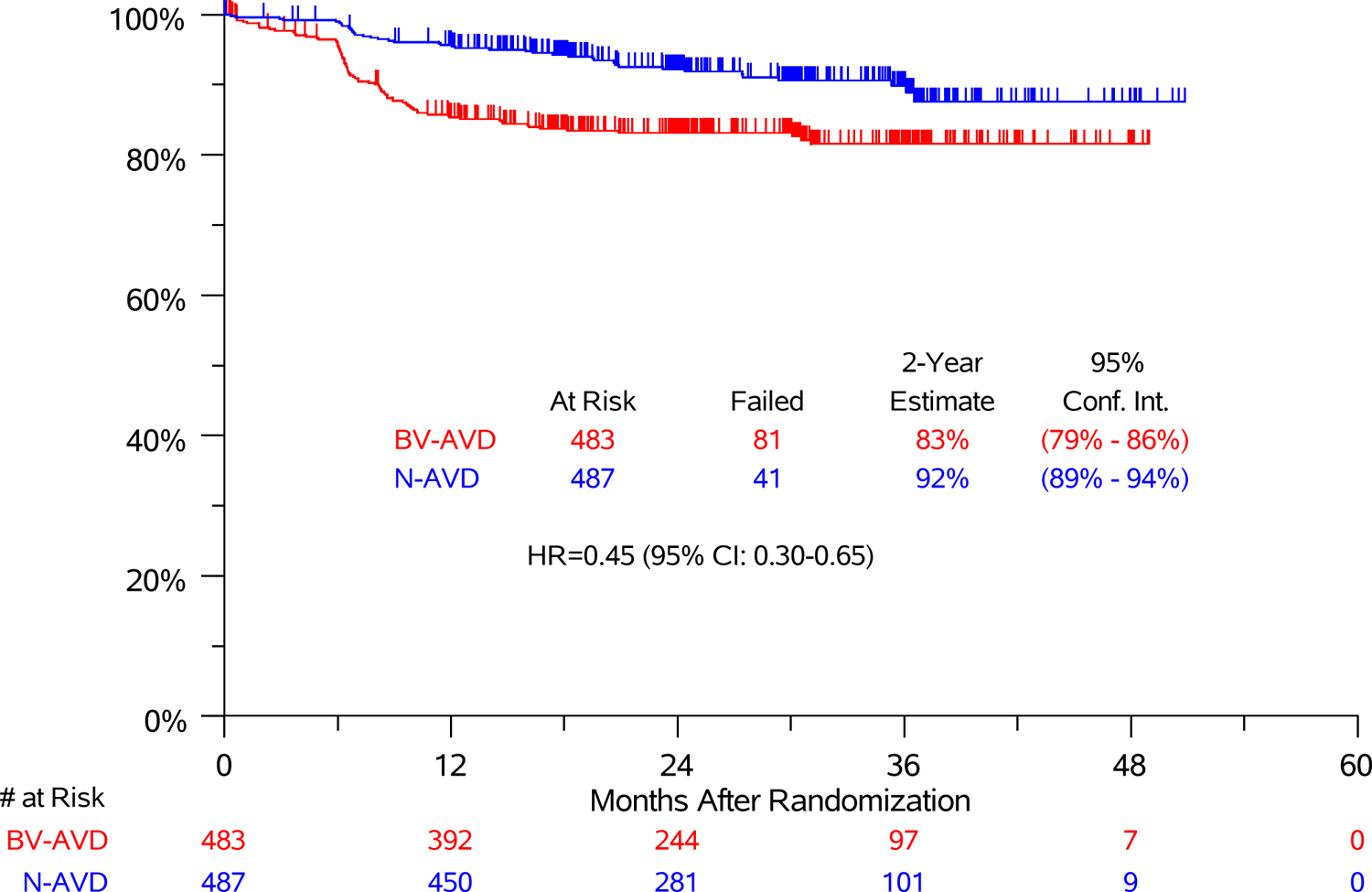
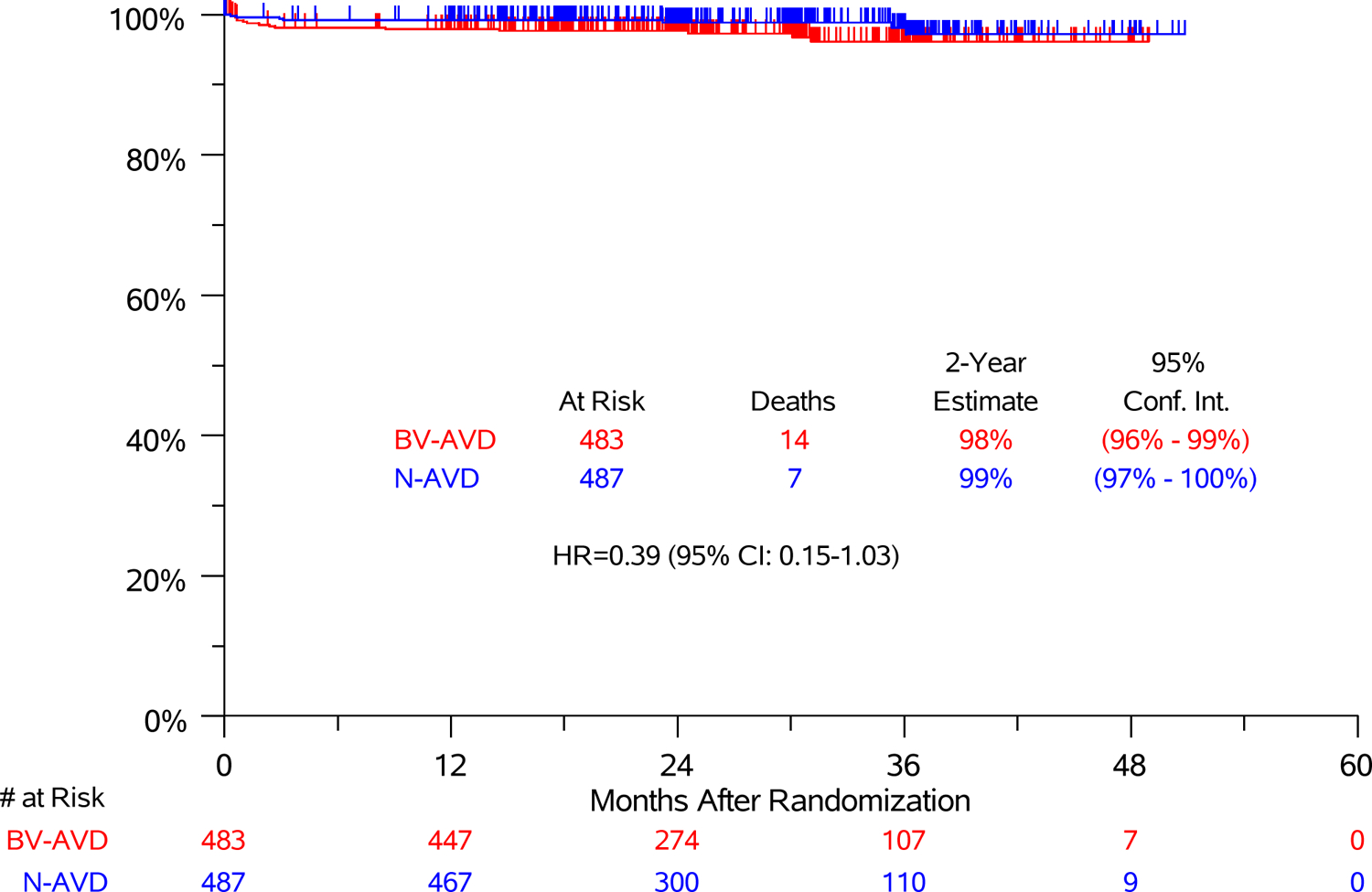
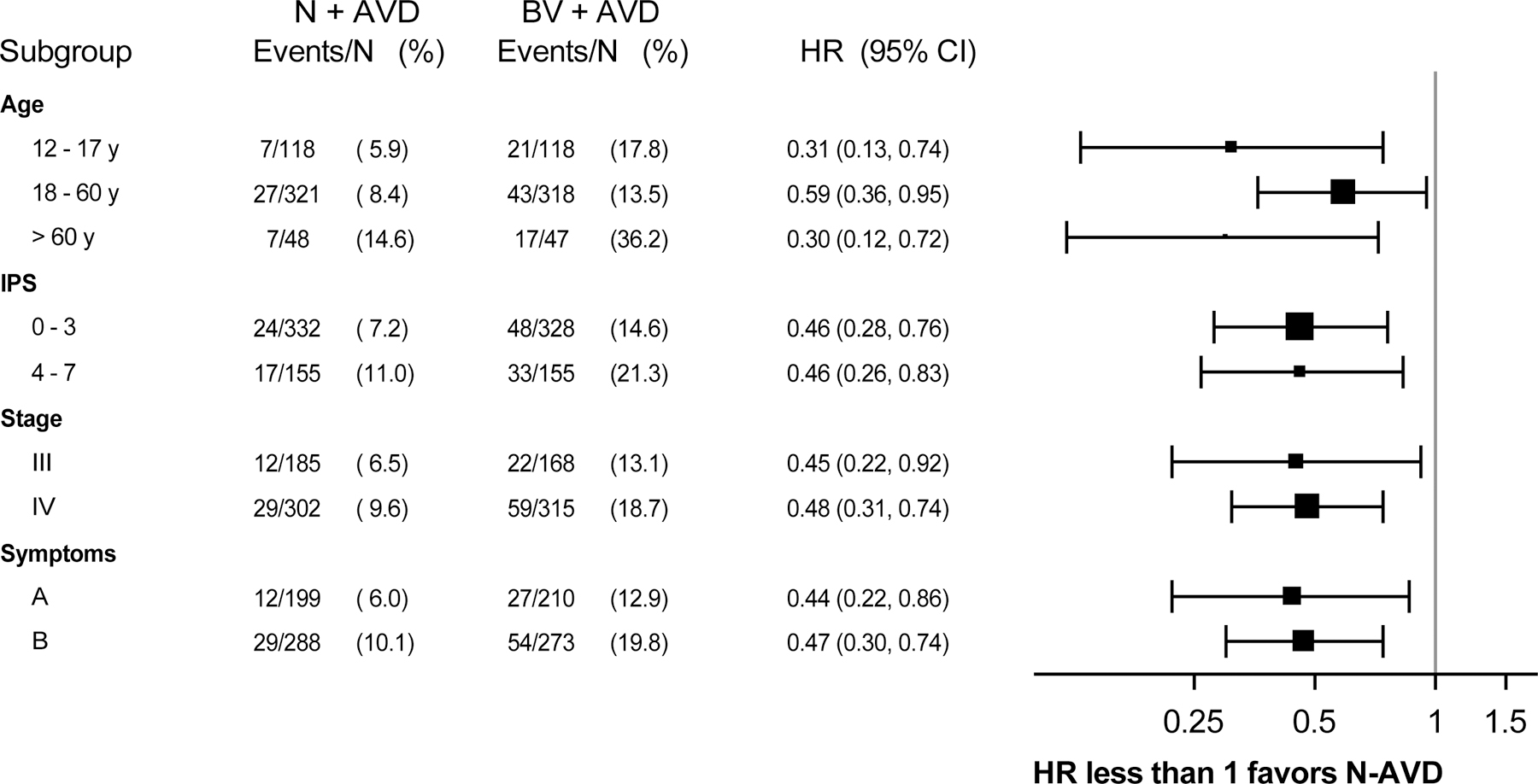
Results: Of 994 patients who underwent randomization, 970 were included in the intention-to-treat population for efficacy analyses. At the second planned interim analysis, with a median follow-up of 12.1 months, the threshold for efficacy was crossed, indicating that N+AVD significantly improved progression-free survival as compared with BV+AVD (hazard ratio for disease progression or death, 0.48; 99% confidence interval [CI], 0.27 to 0.87; two-sided P = 0.001). Owing to the short follow-up time, we repeated the analysis with longer follow-up; with a median follow-up of 2.1 years (range, 0 to 4.2 years), the 2-year progression-free survival was 92% (95% CI, 89 to 94) with N+AVD, as compared with 83% (95% CI, 79 to 86) with BV+AVD (hazard ratio for disease progression or death, 0.45; 95% CI, 0.30 to 0.65). Overall, 7 patients received radiation therapy. Immune-related adverse events were infrequent with nivolumab; brentuximab vedotin was associated with more treatment discontinuation.
Conclusions: N+AVD resulted in longer progression-free survival than BV+AVD in adolescents and adults with stage III or IV advanced-stage classic Hodgkin's lymphoma and had a better side-effect profile. (Funded by the National Cancer Institute of the National Institutes of Health and others; S1826 ClinicalTrials.gov number, NCT03907488.).
Copyright © 2024 Massachusetts Medical Society.
Figures
Comment in
-
Nivolumab+AVD in Advanced-Stage Classic Hodgkin's Lymphoma.N Engl J Med. 2025 Jan 2;392(1):101. doi: 10.1056/NEJMc2414269. N Engl J Med. 2025. PMID: 39752311 No abstract available.
-
Nivolumab+AVD in Advanced-Stage Classic Hodgkin's Lymphoma. Reply.N Engl J Med. 2025 Jan 2;392(1):102. doi: 10.1056/NEJMc2414269. N Engl J Med. 2025. PMID: 39752312 No abstract available.
References
-
- Engert A, Diehl V, Franklin J, et al. Escalated-dose BEACOPP in the treatment of patients with advanced-stage Hodgkin’s lymphoma: 10 years of follow-up of the GHSG HD9 study. J Clin Oncol 2009;27:4548–54. - PubMed
-
- Gordon LI, Hong F, Fisher RI, et al. Randomized phase III trial of ABVD versus Stanford V with or without radiation therapy in locally extensive and advanced-stage Hodgkin lymphoma: an intergroup study coordinated by the Eastern Cooperative Oncology Group (E2496). J Clin Oncol 2013;31:684–91. - PMC - PubMed
-
- Hoppe RT, Advani RH, Ai WZ, et al. NCCN Guidelines(R) Insights: Hodgkin Lymphoma, Version 2.2022. J Natl Compr Canc Netw 2022;20:322–34. - PubMed
-
- Mauz-Korholz C, Hasenclever D, Dorffel W, et al. Procarbazine-free OEPA-COPDAC chemotherapy in boys and standard OPPA-COPP in girls have comparable effectiveness in pediatric Hodgkin’s lymphoma: the GPOH-HD-2002 study. J Clin Oncol 2010;28:3680–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- P30 CA093373/CA/NCI NIH HHS/United States
- UG1CA189955/NH/NIH HHS/United States
- UG1 CA233330/CA/NCI NIH HHS/United States
- U10CA180819/NH/NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- UG1 CA189955/CA/NCI NIH HHS/United States
- U10 CA180863/CA/NCI NIH HHS/United States
- U10CA180863/NH/NIH HHS/United States
- U10CA180888/NH/NIH HHS/United States
- R50 CA285492/CA/NCI NIH HHS/United States
- U10 CA180819/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- R50 CA285409/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10CA180821/NH/NIH HHS/United States
- U10CA180820/NH/NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical