

Predicting mortality in febrile adults: comparative performance of the MEWS, qSOFA, and UVA scores using prospectively collected data among patients in four health-care sites in sub-Saharan Africa and South-Eastern Asia
- PMID: 39416389
- PMCID: PMC11474423
- DOI: 10.1016/j.eclinm.2024.102856
Predicting mortality in febrile adults: comparative performance of the MEWS, qSOFA, and UVA scores using prospectively collected data among patients in four health-care sites in sub-Saharan Africa and South-Eastern Asia
Abstract
Background: Clinical severity scores can identify patients at risk of severe disease and death, and improve patient management. The modified early warning score (MEWS), the quick Sequential (Sepsis-Related) Organ Failure Assessment (qSOFA), and the Universal Vital Assessment (UVA) were developed as risk-stratification tools, but they have not been fully validated in low-resource settings where fever and infectious diseases are frequent reasons for health care seeking. We assessed the performance of MEWS, qSOFA, and UVA in predicting mortality among febrile patients in the Lao PDR, Malawi, Mozambique, and Zimbabwe.
Methods: We prospectively enrolled in- and outpatients aged ≥ 15 years who presented with fever (≥37.5 °C) from June 2018-March 2021. We collected clinical data to calculate each severity score. The primary outcome was mortality 28 days after enrolment. The predictive performance of each score was determined using area under the receiver operating curve (AUC).
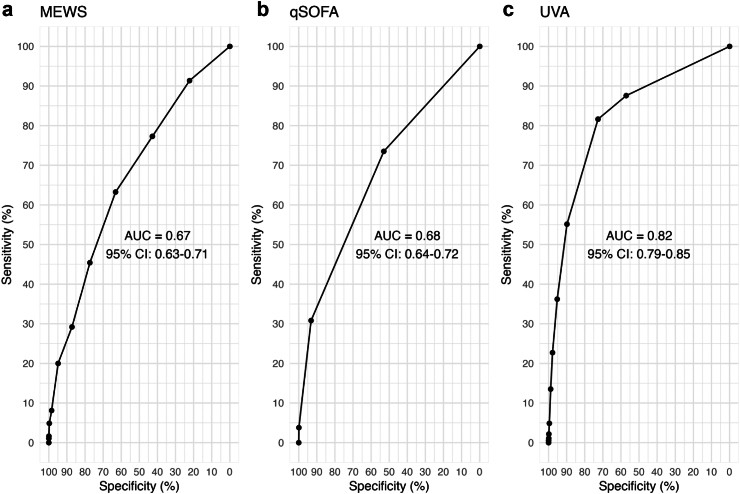
Findings: A total of 2797 participants were included in this analysis. The median (IQR) age was 32 (24-43) years, 38% were inpatients, and 60% (1684/2797) were female. By the time of follow-up, 7% (185/2797) had died. The AUC (95% CI) for MEWS, qSOFA and UVA were 0.67 (0.63-0.71), 0.68 (0.64-0.72), and 0.82 (0.79-0.85), respectively. The AUC comparison found UVA outperformed both MEWS (p < 0.001) and qSOFA (p < 0.001).
Interpretation: We showed that the UVA score performed best in predicting mortality among febrile participants by the time follow-up compared with MEWS and qSOFA, across all four study sites. The UVA score could be a valuable tool for early identification, triage, and initial treatment guidance of high-risk patients in resource-limited clinical settings.
Funding: FCDO.
Keywords: Area under the curve; Fever; MEWS; Mortality; Prognostic scores; Severity scores; UVA; qSOFA.
© 2024 The Author(s).
Conflict of interest statement
HH reports royalties from Wolters Kluwer Health as the primary author and maintainer of the “Laboratory tools for diagnosis of malaria” clinical decision support tool.
Figures


References
-
- Cecconi M., Evans L., Levy M., Rhodes A. Sepsis and septic shock. Lancet. 2018;392:75–87. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
