

Long-term efficacy of mepolizumab in patients with eosinophilic granulomatosis with polyangiitis: a propensity score matching analysis in the multicenter REVEAL cohort study
- PMID: 39416779
- PMCID: PMC11479934
- DOI: 10.3389/fimmu.2024.1457202
Long-term efficacy of mepolizumab in patients with eosinophilic granulomatosis with polyangiitis: a propensity score matching analysis in the multicenter REVEAL cohort study
Abstract
Background: Mepolizumab (MPZ) has demonstrated efficacy in clinical trials for eosinophilic granulomatosis with polyangiitis (EGPA); however, few studies compare the disease course between patients treated with MPZ (MPZ group) and those who were not treated with MPZ (non-MPZ group) in real-world settings.
Objectives: This study aimed to compare the disease course and outcomes between the two groups and assess the long-term efficacy of MPZ in a multicenter cohort in Japan. Methods: We enrolled 113 EGPA patients registered in the cohort until June 2023. Data on clinical characteristics, disease activity, organ damage, treatments, and outcomes were retrospectively collected. To minimize potential confounding factors, we conducted propensity score matching (PSM).
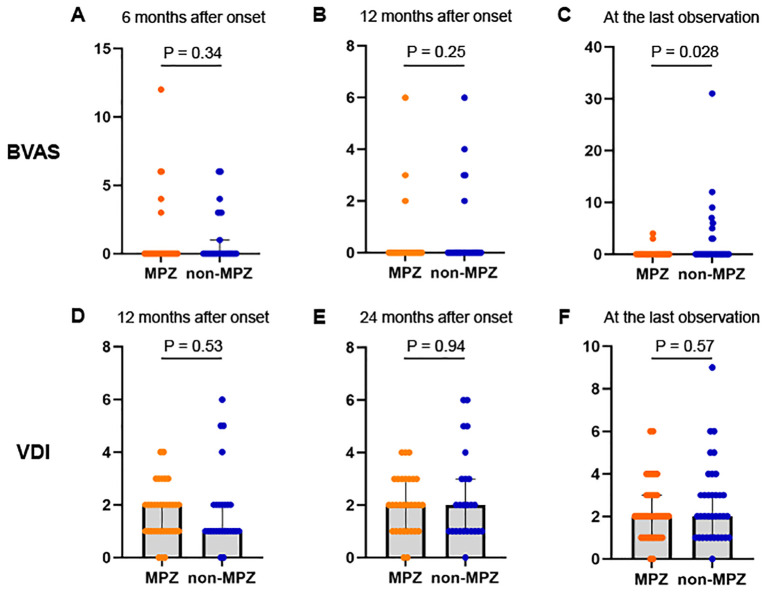
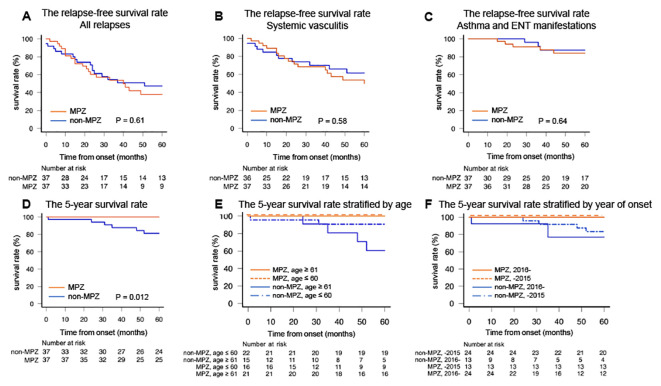
Results: After PSM, 37 pairs of matched patients were identified. Clinical characteristics, including age at disease onset, sex, disease duration at last observation, antineutrophil cytoplasmic antibody positivity at disease onset, Birmingham Vasculitis Activity Score (BVAS) at disease onset, and Five-factor score at disease onset, were comparable between the groups. The median BVAS at the last observation was 0 in both groups; however, more cases in the non-MPZ group exhibited elevated BVAS, resulting in a significantly higher BVAS in the non-MPZ group at the last observation (median; MPZ group: 0, non-MPZ group: 0, p=0.028). The MPZ group had significantly lower glucocorticoid (GC) doses at the last observation (median; MPZ group: 4 mg/day, non-MPZ group: 5 mg/day, p=0.011), with a higher proportion achieving a GC dose ≤ 4 mg/day at the last observation (MPZ group: 51.4%, non-MPZ group: 24.2%, p=0.027). Three models of multivariable logistic regression analyses were performed to identify factors associated with GC doses ≤ 4 mg/day at the last observation. In all models, achieving a GC dose ≤ 4 mg/day was positively associated with MPZ administration and inversely associated with asthma at disease onset. Finally, we evaluated the survival rates between the groups, and the 5-year survival rates were significantly higher in the MPZ group compared to the non-MPZ group (MPZ group: 100%, non-MPZ group: 81.3%, p=0.012).
Conclusion: Mepolizumab not only contributes to disease activity control but also reduces the GC dose, which may lead to improved survival in EGPA patients.
Keywords: eosinophilic granulomatosis with polyangiitis; glucocorticoid-sparing; mepolizumab; multicenter cohort; survival rate.
Copyright © 2024 Shiomi, Watanabe, Matsuda, Kotani, Okazaki, Masuda, Yoshida, Shoji, Tsuge, Kadoba, Hiwa, Yamamoto, Takeda, Itoh and Hashimoto.
Conflict of interest statement
RW received speaker fees from AbbVie, Asahi Kasei, Chugai, Eli Lilly, GSK, and UCB Japan, and research grants from AbbVie. SM received speaker fees from AbbVie, and research grants from Japan Intractable Diseases Research Foundation. TK received speaker fees from AbbVie, Bristol-Myers Squibb, Chugai, Eisai, Eli Lilly, and Pfizer. RH received speaker fees from AbbVie, Asahi Kasei, Bristol-Myers, Daiichi Sankyo, Eisai, Eli Lilly, GSK, Kissei, Pfizer, Tanabe Mitsubishi, and UCB Japan, and research grants from GSK. MH received speaker fees from Bristol Meyers, Chugai, Eisai, Eli Lilly, and Tanabe Mitsubishi, and research grants from AbbVie, Asahi Kasei, Astellas, Bristol Meyers, Eisai, Daiichi Sankyo, Eli Lilly, Novartis Pharma, and Taisho Toyama. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous