

This is a preprint.
Effect of Ventilator Mode on Ventilator-Free Days in Critically Ill Adults: A Randomized Trial
- PMID: 39417127
- PMCID: PMC11483002
- DOI: 10.1101/2024.10.08.24314961
Effect of Ventilator Mode on Ventilator-Free Days in Critically Ill Adults: A Randomized Trial
Update in
-
Effect of Ventilator Mode on Ventilator-Free Days in Critically Ill Adults: A Randomized Clinical Trial.Chest. 2025 Oct;168(4):912-923. doi: 10.1016/j.chest.2025.03.024. Epub 2025 Apr 4. Chest. 2025. PMID: 40189043 Free PMC article. Clinical Trial.
Abstract
Rationale: For critically ill adults receiving invasive mechanical ventilation, the ventilator mode determines how breaths are delivered. Whether the choice of ventilator mode affects outcomes for critically ill patients is unknown. To compare the effects of three common ventilator modes (volume control, pressure control, and adaptive pressure control) on death and duration of mechanical ventilation.
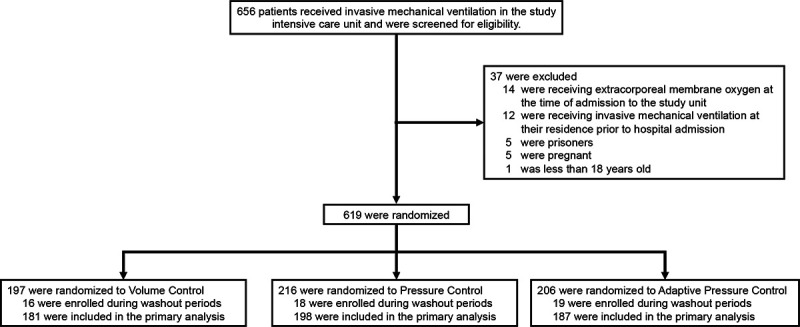
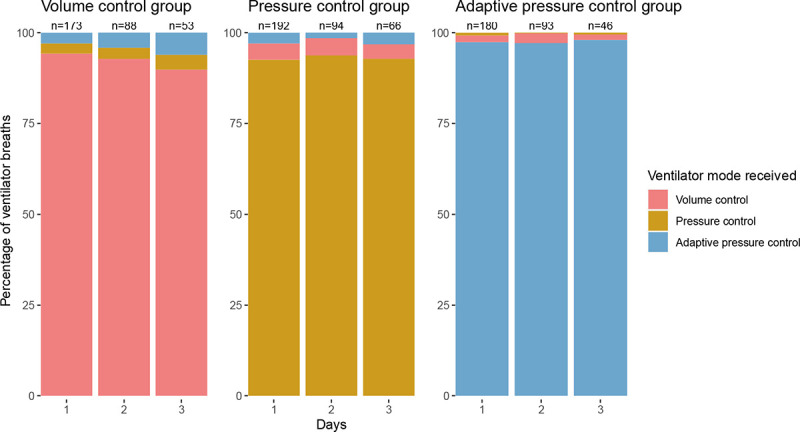
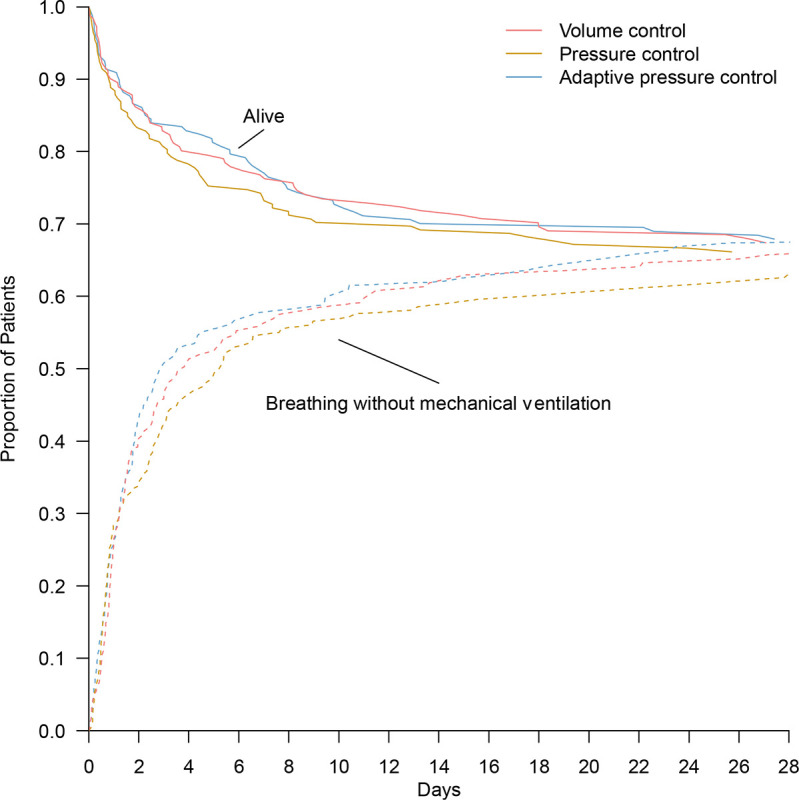
Methods: We conducted a pragmatic, cluster-randomized, crossover trial among adults receiving invasive mechanical ventilation in a medical ICU between November 1, 2022 and July 31, 2023. Each month, patients in the participating unit were assigned to receive volume control, pressure control, or adaptive pressure control during continuous mandatory ventilation. The primary outcome was ventilator-free days through 28 days.
Results: Among 566 patients included in the primary analysis, the median number of ventilator-free days was 23 [IQR, 0-26] in the volume control group, 22 [0-26] in the pressure control group, and 24 [0-26] in the adaptive pressure control group (P=0.60). The median tidal volume was similar in the three groups, but the percentage of breaths larger than 8mL/kg of predicted body weight differed between volume control (median, 4.0%; IQR, 0.0-14.1), pressure control (10.6%; 0.0-31.5), and adaptive pressure control (4.7%; 0.0-19.2). Incidences of hypoxemia, acidemia, and barotrauma were similar in the three groups.
Conclusions: Among critically ill adults receiving invasive mechanical ventilation, the use of volume control, pressure control, or adaptive pressure control did not affect the number of ventilator-free days, however, confidence intervals included differences that may be clinically meaningful.
Keywords: Artificial; Clinical Trial; Critical Illness; Respiration; Respiratory Failure.
Figures
References
-
- Wunsch H, Linde-Zwirble WT, Angus DC, Hartman ME, Milbrandt EB, Kahn JM. The epidemiology of mechanical ventilation use in the United States*: Critical Care Medicine 2010;38(10):1947–53. - PubMed
-
- Dreyfuss D, Saumon G. Ventilator-induced Lung Injury: Lessons from Experimental Studies. Am J Respir Crit Care Med 1998;157(1):294–323. - PubMed
-
- Vassilakopoulos T, Petrof BJ. Ventilator-induced Diaphragmatic Dysfunction. Am J Respir Crit Care Med 2004;169(3):336–41. - PubMed
-
- Slutsky AS, Ranieri VM. Ventilator-Induced Lung Injury. N Engl J Med 2013;369(22):2126–36. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources