

Exercise cardiovascular magnetic resonance shows improved diastolic filling by atrioventricular area difference in athletes and controls
- PMID: 39417822
- PMCID: PMC11687837
- DOI: 10.1152/japplphysiol.00446.2024
Exercise cardiovascular magnetic resonance shows improved diastolic filling by atrioventricular area difference in athletes and controls
Abstract
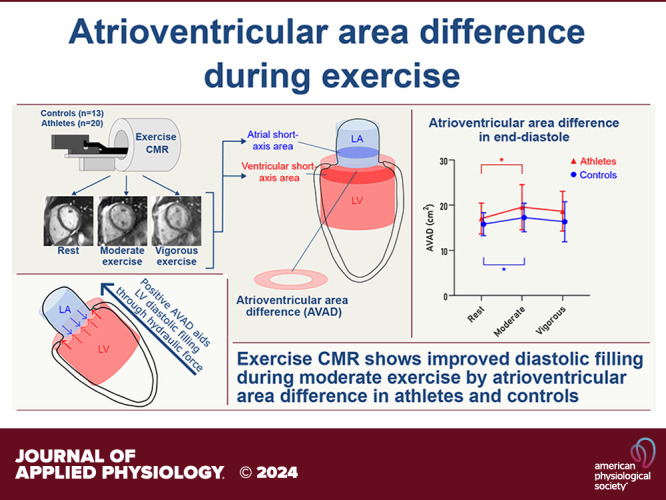
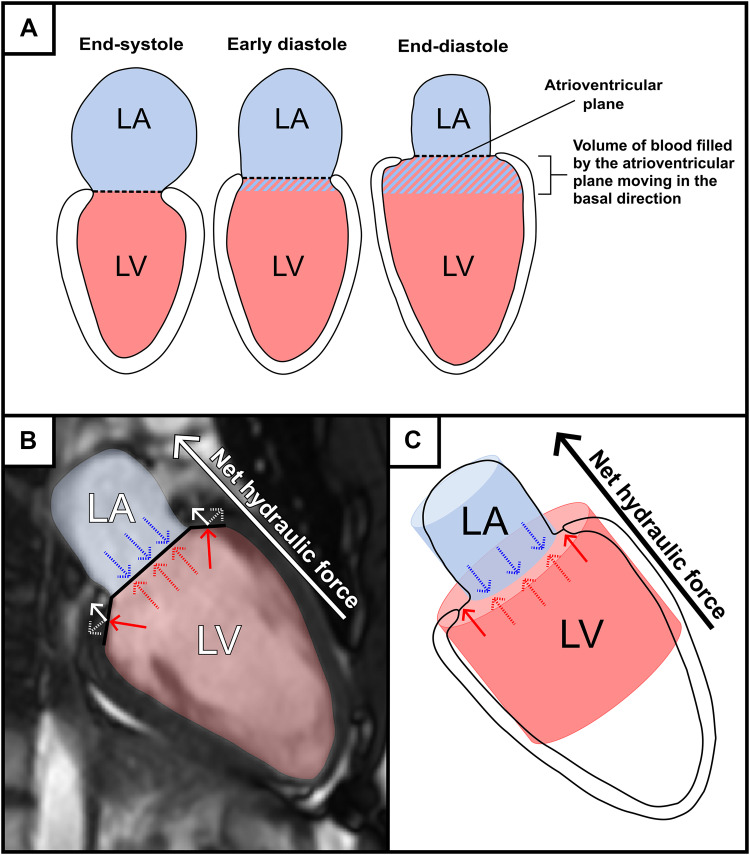
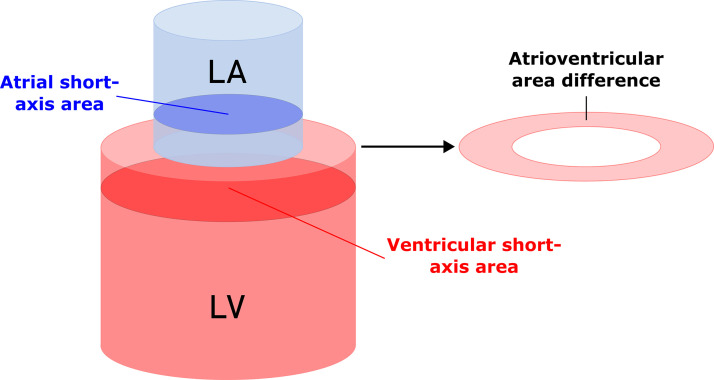
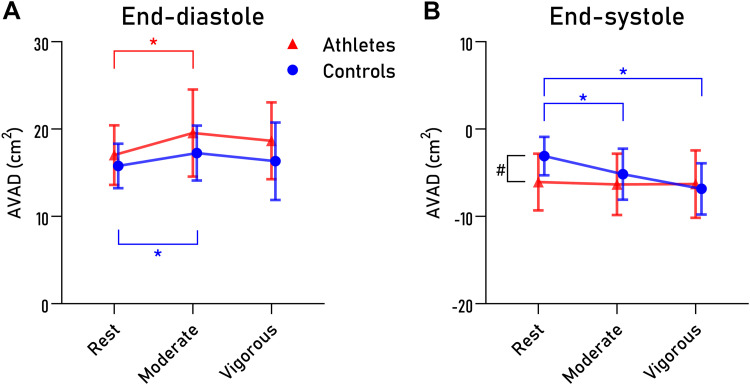
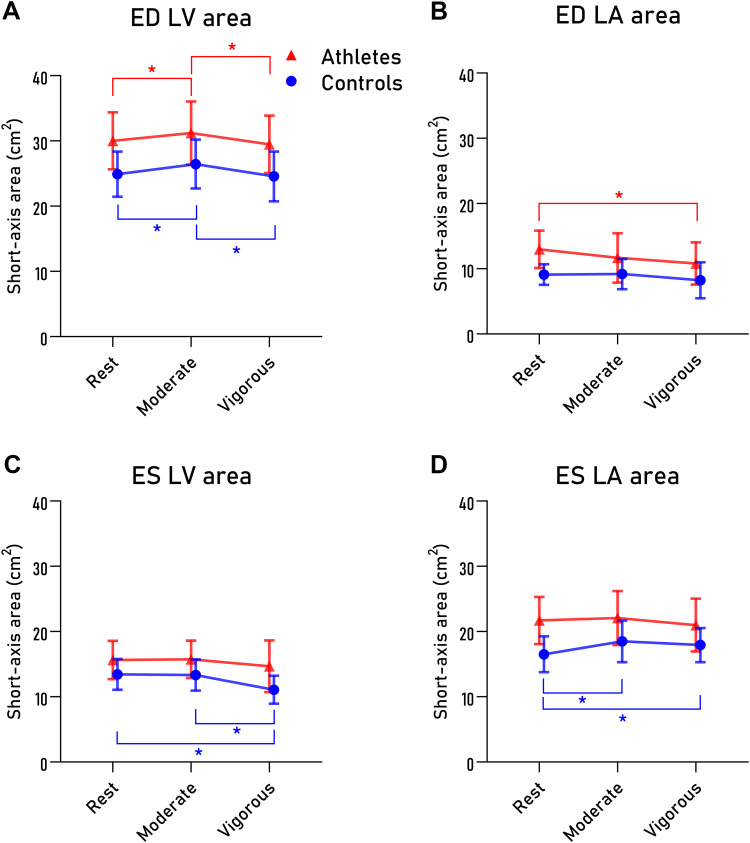
Hydraulic force, a novel mechanism shown to aid diastolic filling, can be calculated by assessing the geometrical relationship between the left ventricular and atrial short-axis areas (atrioventricular area difference, AVAD) (Maksuti E, Carlsson M, Arheden H, Kovács SJ, Broomé M, Ugander M. Sci Rep 7: 43505-43510, 2017; Steding-Ehrenborg K, Hedström E, Carlsson M, Maksuti E, Broomé M, Ugander M, Magnusson M, Smith JG, Arheden H. J Appl Physiol (1985) 130: 993-1000, 2021). During exercise both ventricular and atrial volumes change due to altered loading conditions compared with rest, but it is unknown to what extent this affects AVAD. The aim of this study was to investigate whether AVAD differs when going from rest to exercise in sedentary controls and athletes. We included 13 sedentary controls and 20 endurance athletes to undergo cardiovascular magnetic resonance (CMR) imaging at rest and during moderate and vigorous exercise using a CMR-compatible ergometer. AVAD was calculated as the largest ventricular short-axis area minus the largest atrial short-axis area in end-diastole (ED) and end-systole (ES) as measured from CMR short-axis images. AVAD in ED increased during moderate exercise in both sedentary controls and athletes, thus aiding diastolic filling, but did not increase further during vigorous exercise. AVAD in ES was negative in both groups at rest and decreased further with increasing exercise intensity in sedentary controls, whereas athletes remained unchanged. In conclusion, results from AVAD in ED indicate the net hydraulic force to further augment diastolic filling during moderate exercise when compared with rest, providing new insights into the mechanism by which diastolic function increases during exercise.NEW & NOTEWORTHY This study is the first to assess hydraulic force during exercise, a novel mechanism shown to augment diastolic filling at rest. Our results indicate hydraulic force to further aid in diastolic filling during moderate exercise compared with rest in athletes and sedentary controls, providing new insights into the mechanism by which the left ventricle increases diastolic function during exercise.
Keywords: atrioventricular area difference; exercise cardiac magnetic resonance imaging; hydraulic force; left atrium; left ventricle.
Conflict of interest statement
Einar Heiberg is the founder of software company Medviso AB, which develops the software Segment that was used in the image analysis in the current study. None of the other authors has any conflicts of interest, financial or otherwise, to disclose.
Figures
References
-
- La Gerche A, Claessen G, Van de Bruaene A, Pattyn N, Van Cleemput J, Gewillig M, Bogaert J, Dymarkowski S, Claus P, Heidbuchel H. Cardiac MRI: a new gold standard for ventricular volume quantification during high-intensity exercise. Circ Cardiovasc Imaging 6: 329–338, 2013. doi: 10.1161/CIRCIMAGING.112.980037. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical