

Fluid balance neutralization secured by hemodynamic monitoring versus protocolized standard of care in patients with acute circulatory failure requiring continuous renal replacement therapy: results of the GO NEUTRAL randomized controlled trial
- PMID: 39417870
- PMCID: PMC11588767
- DOI: 10.1007/s00134-024-07676-1
Fluid balance neutralization secured by hemodynamic monitoring versus protocolized standard of care in patients with acute circulatory failure requiring continuous renal replacement therapy: results of the GO NEUTRAL randomized controlled trial
Abstract
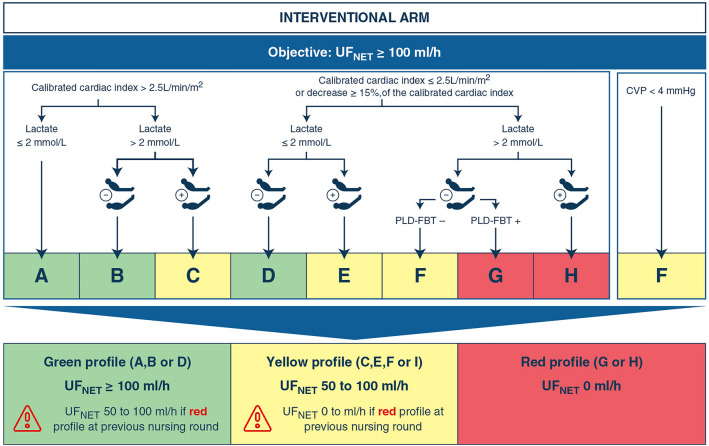
Purpose: Net ultrafiltration (UFNET) during continuous renal replacement therapy (CRRT) can control fluid balance (FB), but is usually 0 ml·h-1 in patients with vasopressors due to the risk of hemodynamic instability associated with CRRT (HIRRT). We evaluated a UFNET strategy adjusted by functional hemodynamics to control the FB of patients with vasopressors, compared to the standard of care.
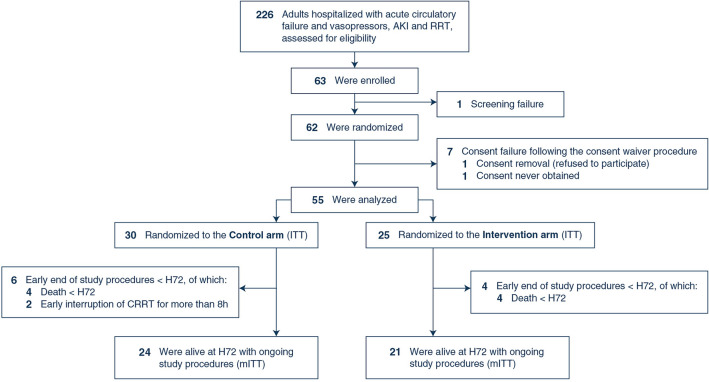
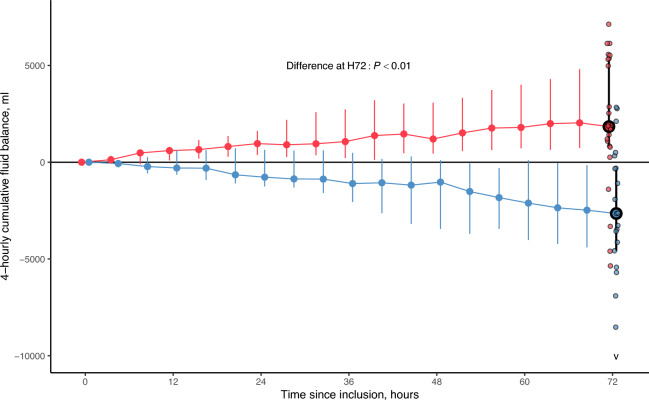
Methods: In this randomized, controlled, open-label, parallel-group, multicenter, proof-of-concept trial, adults receiving vasopressors, CRRT since ≤ 24 h and cardiac output monitoring were randomized (ratio 1:1) to receive during 72 h a UFNET ≥ 100 ml·h-1, adjusted using a functional hemodynamic protocol (intervention), or a UFNET ≤ 25 ml·h-1 (control). The primary outcome was the cumulative FB at 72 h and was analyzed in patients alive at 72 h and in whom monitoring and CRRT were continuously provided (modified intention-to-treat population [mITT]). Secondary outcomes were analyzed in the intention-to-treat (ITT) population.
Results: Between June 2021 and April 2023, 55 patients (age 69 [interquartile range, IQR: 62; 74], 35% female, Sequential Organ Failure Assessment (SOFA) 13 [11; 15]) were randomized (25 interventions, 30 controls). In the mITT population, (21 interventions, 24 controls), the 72 h FB was -2650 [-4574; -309] ml in the intervention arm, and 1841 [821; 5327] ml in controls (difference: 4942 [95% confidence interval: 2736-6902] ml, P < 0.01). Hemodynamics, oxygenation and the number of HIRRT at 72 h, and day-90 mortality did not statistically differ between arms.
Conclusion: In patients with vasopressors, a UFNET fluid removal strategy secured by a hemodynamic protocol allowed active fluid balance control, compared to the standard of care.
Keywords: Acute circulatory failure; Continuous renal replacement therapy; Fluid balance; Functional hemodynamics; Pulse contour; Transpulmonary thermodilution.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: LB is the recipient of the study’s funding grant from the Programme Hospitalier de Recherche Clinique Inter-régional (PHRC-I 2019) from the Direction Générale de l’Offre de Soin (French Ministry of Health). JI declares registration and travel fees for congress attendance payed by Pfizer. J-CR declares registration and travel fees for congress attendance payed by Pfizer. All other authors declare no competing interests. Ethical approval: The study was conducted in accordance with the Declaration of Helsinki and with local regulations. The study was registered at ClinicalTrials.gov (NCT04801784) before the first patient was enrolled. The study protocol was reviewed and approved by an ethics committee for human research (Comité de Protection des Personnes Sud Méditerranée I, IDCRB 2021-A00692-39).
Figures
References
-
- Schortgen F, Tabra Osorio C, Carpentier D, Henry M, Beuret P, Lacave G, Simon G, Blanchard PY, Gobe T, Guillon A, Bitker L, Duhommet G, Quenot JP, Le Meur M, Jochmans S, Dubouloz F, Mainguy N, Saletes J, Creutin T, Nicolas P, Senay J, Berthelot AL, Rizk D, Van Tran D, Riviere A, Heili-Frades SB, Nunes J, Robquin N, Lhotellier S, Ledochowski S, Guenegou-Arnoux A, Constan A (2023) Fluid intake in critically ill patients: the “save useless fluids for intensive resuscitation” multicenter prospective cohort study. Crit Care Med 52:258–267 - PubMed
-
- Messmer AS, Zingg C, Muller M, Gerber JL, Schefold JC, Pfortmueller CA (2020) Fluid overload and mortality in adult critical care patients-a systematic review and meta-analysis of observational studies. Crit Care Med 48:1862–1870 - PubMed
-
- Vaara ST, Korhonen AM, Kaukonen KM, Nisula S, Inkinen O, Hoppu S, Laurila JJ, Mildh L, Reinikainen M, Lund V, Parviainen I, Pettila V, Group FS (2012) Fluid overload is associated with an increased risk for 90-day mortality in critically ill patients with renal replacement therapy: data from the prospective FINNAKI study. Crit care 16:R197 - PMC - PubMed
-
- Woodward CW, Lambert J, Ortiz-Soriano V, Li Y, Ruiz-Conejo M, Bissell BD, Kelly A, Adams P, Yessayan L, Morris PE, Neyra JA (2019) Fluid overload associates with major adverse kidney events in critically ill patients with acute kidney injury requiring continuous renal replacement therapy. Crit Care Med 47:e753–e760 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
