

Mass incarceration as a driver of the tuberculosis epidemic in Latin America and projected effects of policy alternatives: a mathematical modelling study
- PMID: 39419058
- PMCID: PMC11602220
- DOI: 10.1016/S2468-2667(24)00192-0
Mass incarceration as a driver of the tuberculosis epidemic in Latin America and projected effects of policy alternatives: a mathematical modelling study
Abstract
Background: Tuberculosis incidence is increasing in Latin America, where the incarcerated population has nearly quadrupled since 1990. We aimed to quantify the impact of historical and future incarceration policies on the tuberculosis epidemic, accounting for effects in and beyond prisons.
Methods: In this modelling study, we calibrated dynamic compartmental transmission models to historical and contemporary data from Argentina, Brazil, Colombia, El Salvador, Mexico, and Peru, which comprise approximately 80% of the region's incarcerated population and tuberculosis burden. The model was fit independently for each country to incarceration and tuberculosis data from 1990 to 2023 (specific dates were country dependent). The model does not include HIV, drug resistance, gender or sex, or age structure. Using historical counterfactual scenarios, we estimated the transmission population attributable fraction (tPAF) for incarceration and the excess population-level burden attributable to increasing incarceration prevalence since 1990. We additionally projected the effect of alternative incarceration policies on future population tuberculosis incidence.
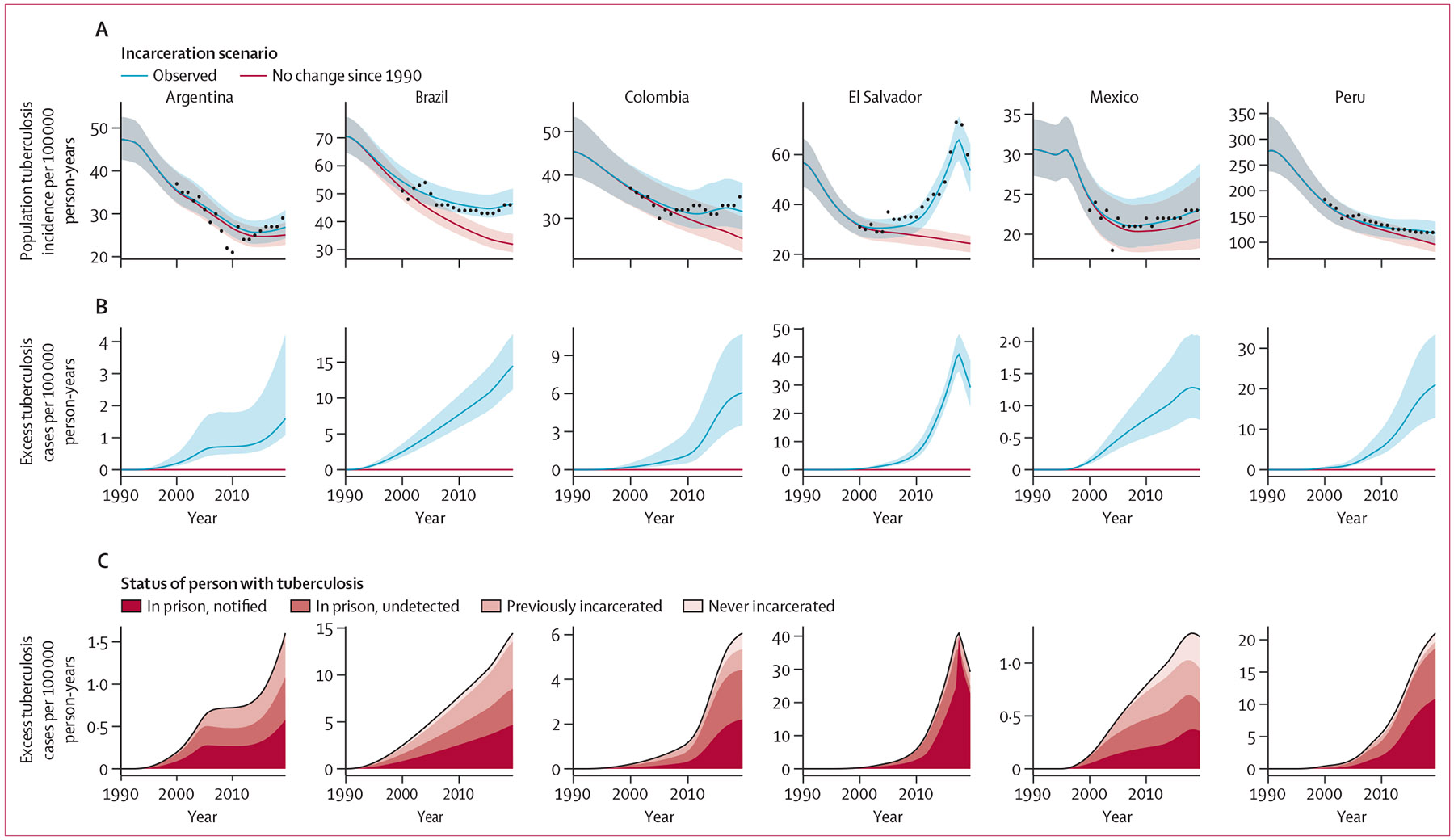
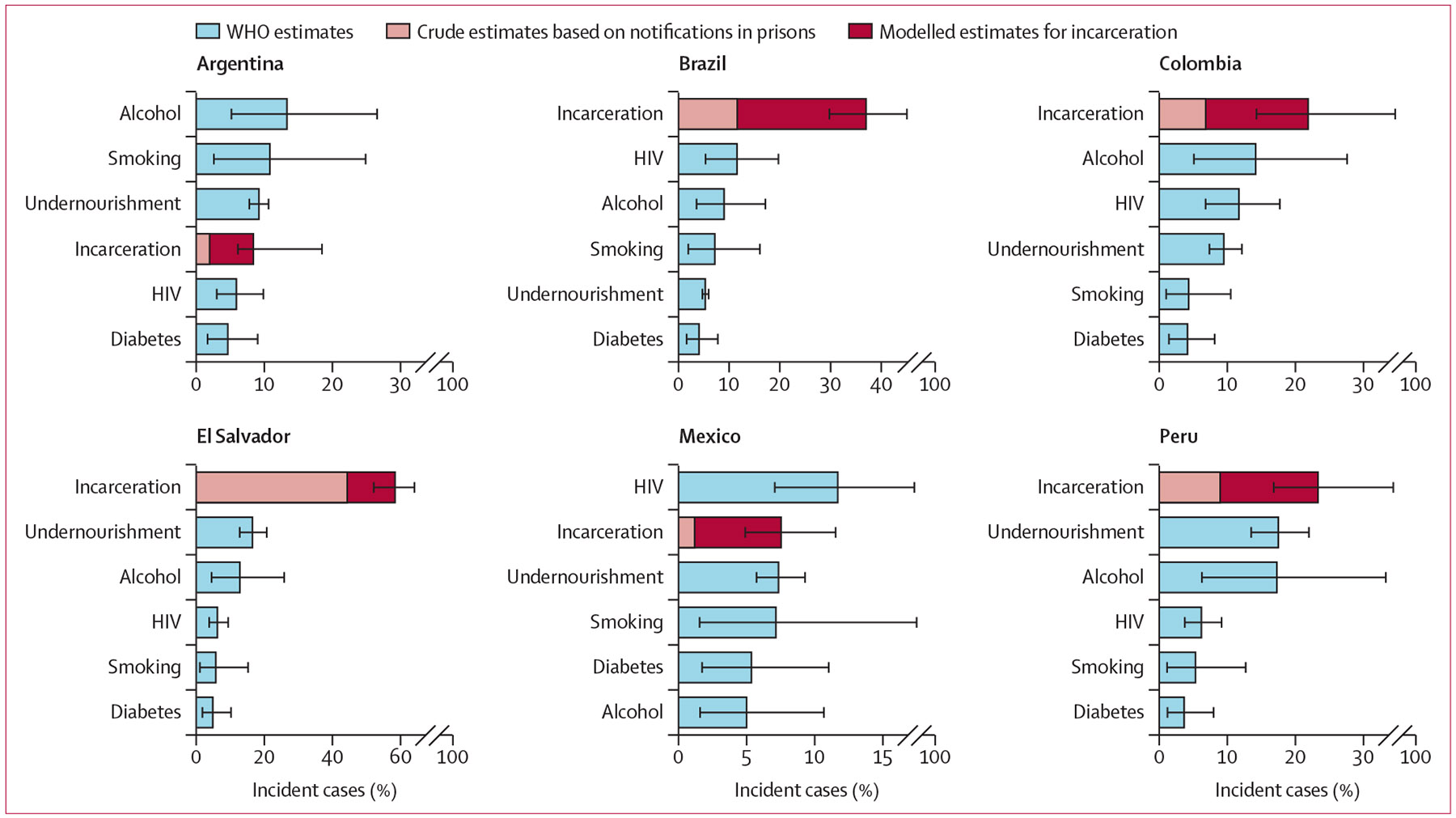
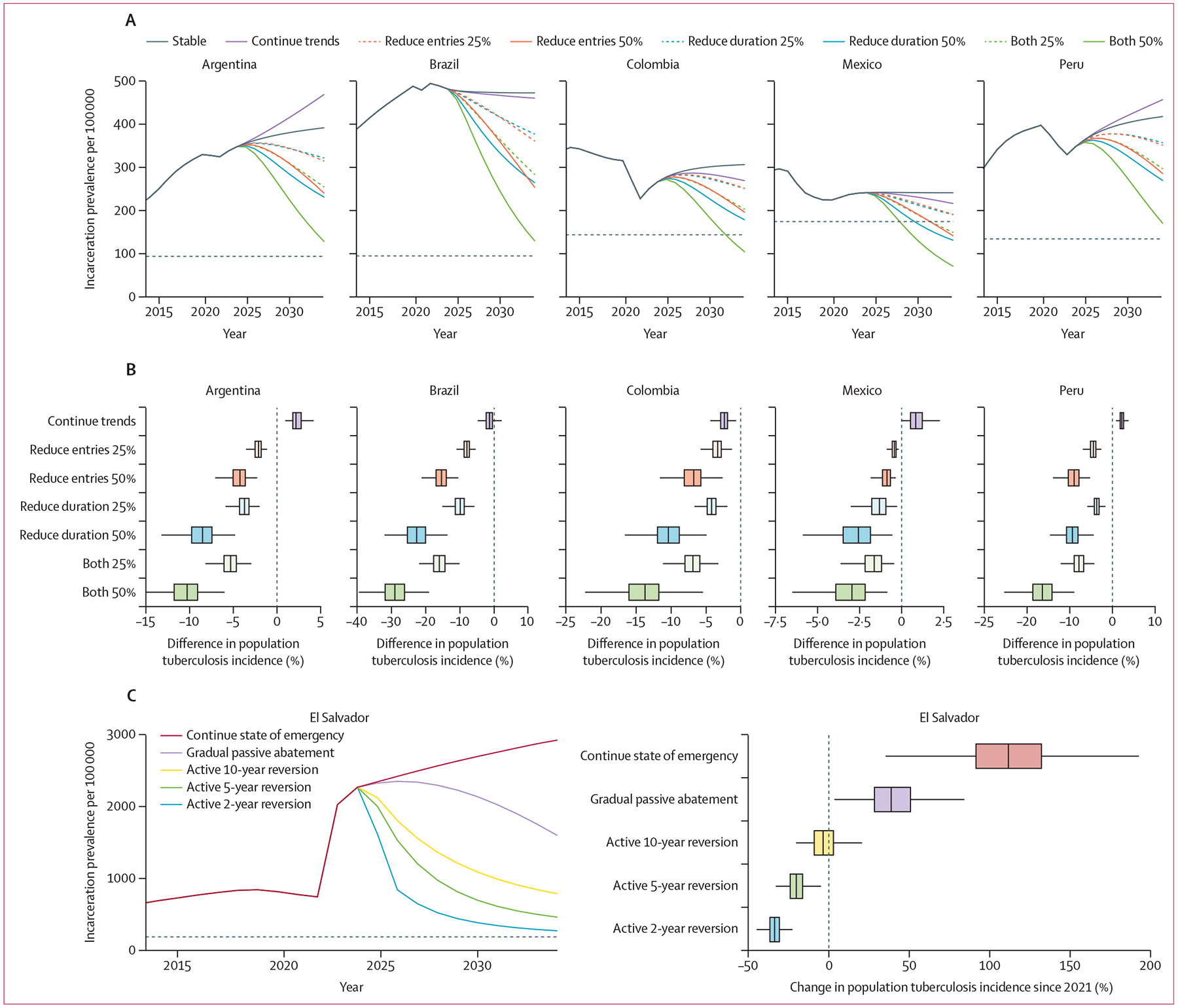
Findings: Population tuberculosis incidence in 2019 was 29·4% (95% uncertainty interval [UI] 23·9-36·8) higher than expected without the rise in incarceration since 1990, corresponding to 34 393 (28 295-42 579) excess incident cases across countries. The incarceration tPAF in 2019 was 27·2% (20·9-35·8), exceeding estimates for other risk factors like HIV, alcohol use disorder, and undernutrition. Compared with a scenario where incarceration rates remain stable at current levels, a gradual 50% reduction in prison admissions and duration of incarceration by 2034 would reduce population tuberculosis incidence by over 10% in all countries except Mexico.
Interpretation: The historical rise in incarceration in Latin America has resulted in a large excess tuberculosis burden that has been under-recognised to date. International health agencies, ministries of justice, and national tuberculosis programmes should collaborate to address this health crisis with comprehensive strategies, including decarceration.
Funding: National Institutes of Health.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests YEL reports funding from the Stanford Knight Hennessy Scholars Program, the National Science Foundation Graduate Research Fellowship, and the Gerald J Lieberman Fellowship from the Stanford Office of the Vice Provost for Graduate Education; and a previous leadership role in the Stanford Jail and Prison Education Program. MAH reports grants or contracts paid to their institution from the National Institutes of Health (NIH), Gilead Sciences, Insmed, AN2 Therapeutics, and AstraZeneca; and participation on the AIDS Clinical Trials Group Tuberculosis Transformative Science Group Study Monitoring Committee. TC reports grants from the Centers for Disease Control and Prevention and NIH to their institution. JC reports grants or contracts from Valneva–Instituto Butantan, Merck & Co, Sanofi Pasteur, Coalition for Epidemic Preparedness Innovations–Sabin Vaccine Institute, and Takeda; speaking fees from Pfizer; and participation in Advisory Boards for the mRNA-1273 vaccine (for Moderna–Zodiac), RSV maternal vaccine (for Pfizer), Qdenga vaccine (for Takeda), Nirmatrelvir–Ritonavir (for Paxlovid and Pfizer), and the Global Dengue Steering Committee (for Takeda). JRA reports grants from Good Ventures–Open Philanthropy for an ethics evaluation of tuberculosis vaccine trials paid to their institution; payment for expert testimony involving tuberculosis in prisons in the USA; participation on safety monitoring boards and advisory boards for NIH-sponsored clinical studies and trials pertaining to tuberculosis; a leadership role in the TB in Prisons Working Group for the International Union Against Tuberculosis and Lung Disease; and a donation of materials from Cepheid for research use. All other authors declare no competing interests.
Figures
Update of
-
Mass incarceration as a driver of the tuberculosis epidemic in Latin America and projected impacts of policy alternatives: A mathematical modeling study.medRxiv [Preprint]. 2024 Jul 22:2024.04.23.24306238. doi: 10.1101/2024.04.23.24306238. medRxiv. 2024. Update in: Lancet Public Health. 2024 Nov;9(11):e841-e851. doi: 10.1016/S2468-2667(24)00192-0. PMID: 39108530 Free PMC article. Updated. Preprint.
References
-
- WHO. Global tuberculosis report 2023. Geneva: World Health Organization, 2023.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
