

Burden of postmenopausal breast cancer attributable to excess body weight: comparative study of body mass index and CUN-BAE in MCC-Spain study
- PMID: 39419524
- PMCID: PMC11671986
- DOI: 10.1136/jech-2023-220706
Burden of postmenopausal breast cancer attributable to excess body weight: comparative study of body mass index and CUN-BAE in MCC-Spain study
Abstract
Background: 10% of postmenopausal breast cancer cases are attributed to a high body mass index (BMI). BMI underestimates body fat, particularly in older women, and therefore the cancer burden attributable to obesity may be even higher. However, this is not clear. CUN-BAE (Clínica Universidad de Navarra-Body Adiposity Estimator) is an accurate validated estimator of body fat, taking into account sex and age. The objective of this study was to compare the burden of postmenopausal breast cancer attributable to excess body fat calculated using BMI and CUN-BAE.
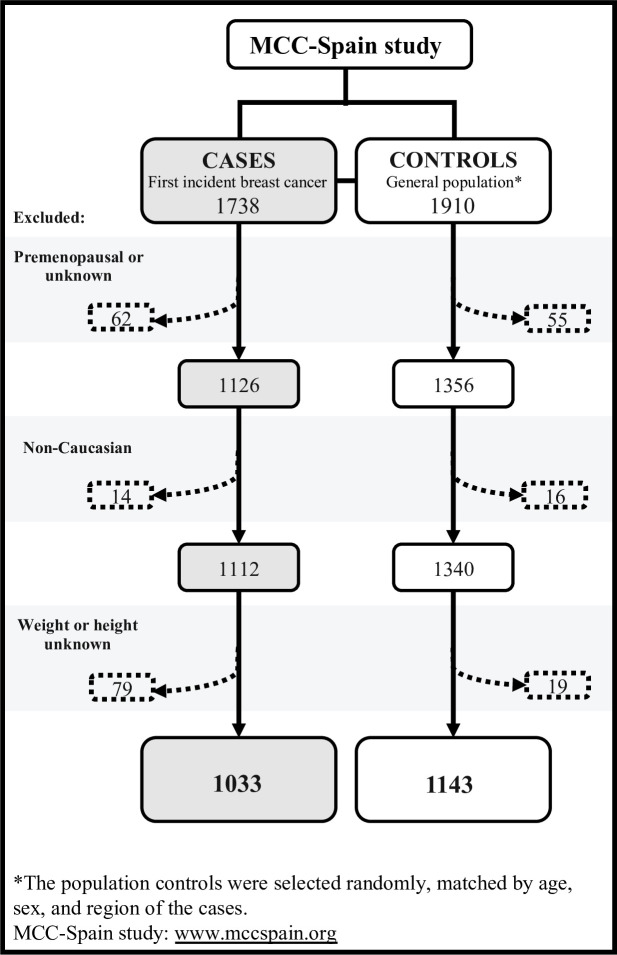
Methods: This case-control study included 1033 cases of breast cancer and 1143 postmenopausal population controls from the multicase-control MCC-Spain study. Logistic regression models were used to calculate odds ratios (ORs). The population attributable fraction (PAF) of excess weight related to breast cancer was estimated with both anthropometric measures. Stratified analyses were carried out for hormone receptor type.
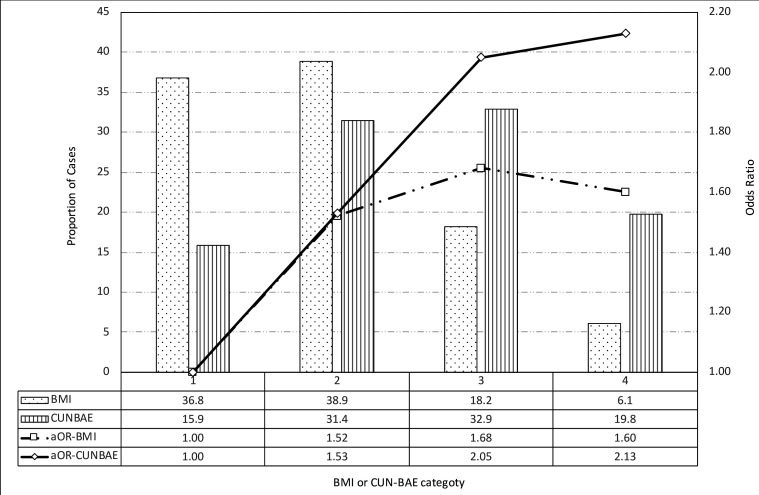
Results: Excess body weight attributable to the risk of breast cancer was 23.0% when assessed using a BMI value ≥30 kg/m2 and 38.0% when assessed using a CUN-BAE value of ≥40% body fat. Hormone receptor stratification showed that these differences in PAFs were only observed in hormone receptor positive cases, with an estimated burden of 19.9% for BMI and 41.9% for CUN-BAE.
Conclusion: These findings suggest that the significance of excess body fat in postmenopausal hormone receptor positive breast cancer could be underestimated when assessed using only BMI. Accurate estimation of the cancer burden attributable to obesity is crucial for planning effective prevention initiatives.
Keywords: BREAST NEOPLASMS; HEALTH IMPACT ASSESSMENT; OBESITY.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Cancer Research Fund / American Institute of Cancer Research . London: 2018. [5-Jun-2018]. Third expert report. Diet, nutrition, physical activity and cancer: a global perspective. continuous update project report.https://www.wcrf.org/dietandcancer Available. accessed.