

Systolic blood pressure variability in late-life predicts cognitive trajectory and risk of Alzheimer's disease
- PMID: 39420926
- PMCID: PMC11483855
- DOI: 10.3389/fnagi.2024.1448034
Systolic blood pressure variability in late-life predicts cognitive trajectory and risk of Alzheimer's disease
Abstract
Background: The relationship of systolic blood pressure variability (SBPV) with Alzheimer's disease (AD) remains controversial. We aimed to explore the roles of SBPV in predicting AD incidence and to test the pathways that mediated the relationship of SBPV with cognitive functions.
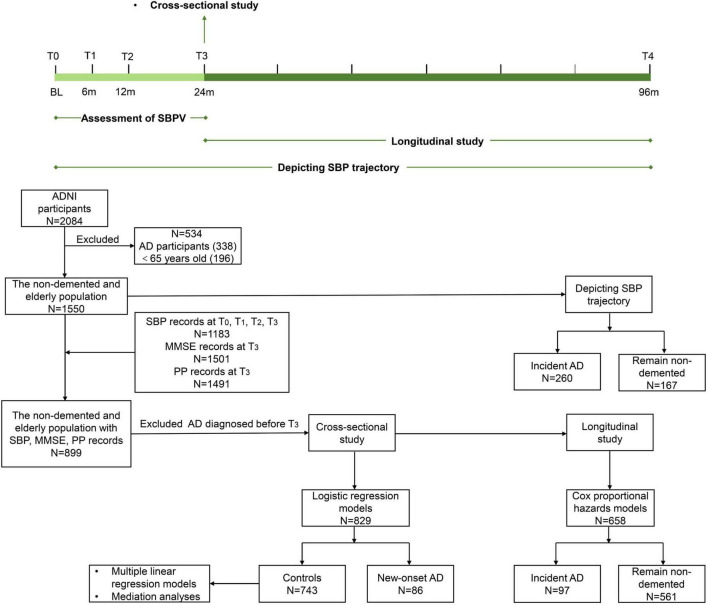
Methods: Longitudinal data across 96 months (T0 to T4) were derived from the Alzheimer's disease Neuroimaging Initiative cohort. SBPV for each participant was calculated based on the four measurements of SBP across 24 months (T0 to T3). At T3, logistic regression models were used to test the SBPV difference between 86 new-onset AD and 743 controls. Linear regression models were used to test the associations of SBPV with cognition and AD imaging endophenotypes for 743 non-demented participants (median age = 77.0, female = 42%). Causal mediation analyses were conducted to explore the effects of imaging endophenotypes in mediating the relationships of SBPV with cognitive function. Finally, Cox proportional hazard model was utilized to explore the association of SBPV with incident risk of AD (T3 to T4, mean follow-up = 3.5 years).
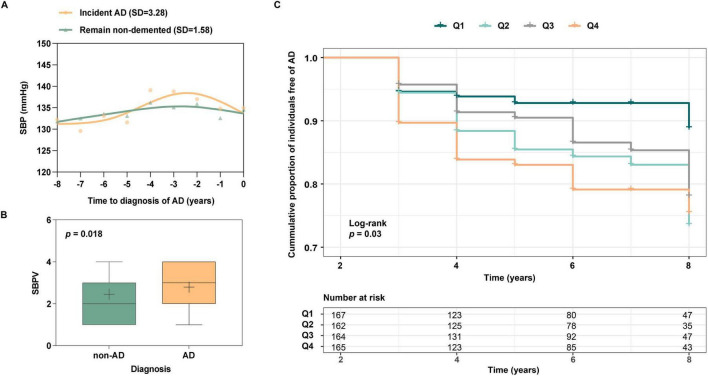
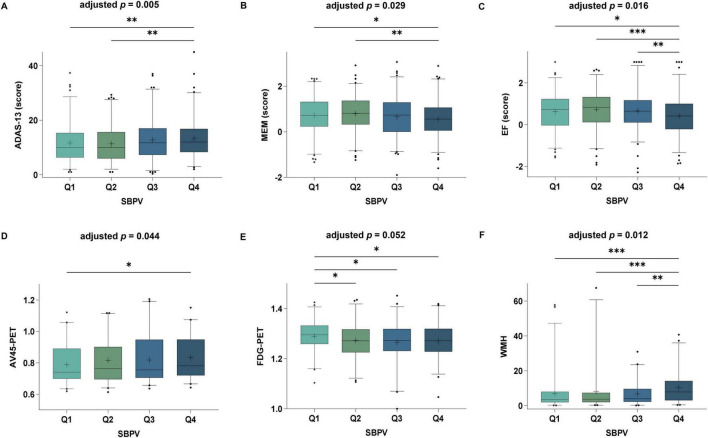
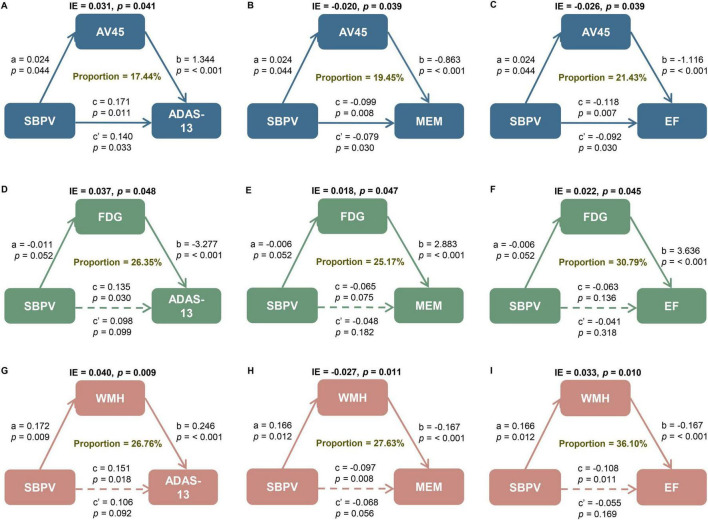
Results: Participants with new-onset AD at T3 had significantly higher SBPV compared to their controls (p = 0.018). Higher SBPV was associated with lower scores of cognitive function (p = 0.005 for general cognition, p = 0.029 for memory, and p = 0.016 for executive function), higher cerebral burden of amyloid deposition by AV45 PET (p = 0.044), lower brain metabolism by FDG PET (p = 0.052), and higher burden of white matter hyperintensities (WMH) (p = 0.012). Amyloid pathology, brain metabolism, and WMH partially (ranging from 17.44% to 36.10%) mediated the associations of SBPV with cognition. Higher SBPV was significantly associated with elevated risk of developing AD (hazard ratio = 1.29, 95% confidence interval = 1.07 to 1.57, p = 0.008).
Conclusion: These findings supported that maintaining stable SBP in late life helped lower the risk of AD, partially by modulating amyloid pathology, cerebral metabolism, and cerebrovascular health.
Keywords: Alzheimer’s disease; amyloid; brain metabolism; systolic blood pressure variability; white matter hyperintensities.
Copyright © 2024 Li, Wang, Tan, Tan and Xu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Topographic patterns of white matter hyperintensities are associated with multimodal neuroimaging biomarkers of Alzheimer's disease.Alzheimers Res Ther. 2021 Jan 18;13(1):29. doi: 10.1186/s13195-020-00759-3. Alzheimers Res Ther. 2021. PMID: 33461618 Free PMC article.
-
The relationship between amyloid pathology, cerebral small vessel disease, glymphatic dysfunction, and cognition: a study based on Alzheimer's disease continuum participants.Alzheimers Res Ther. 2024 Feb 20;16(1):43. doi: 10.1186/s13195-024-01407-w. Alzheimers Res Ther. 2024. PMID: 38378607 Free PMC article.
-
White matter hyperintensities and cognition across different Alzheimer's biomarker profiles.J Am Geriatr Soc. 2021 Jul;69(7):1906-1915. doi: 10.1111/jgs.17173. Epub 2021 Apr 23. J Am Geriatr Soc. 2021. PMID: 33891712 Free PMC article.
-
Understanding disease progression and improving Alzheimer's disease clinical trials: Recent highlights from the Alzheimer's Disease Neuroimaging Initiative.Alzheimers Dement. 2019 Jan;15(1):106-152. doi: 10.1016/j.jalz.2018.08.005. Epub 2018 Oct 13. Alzheimers Dement. 2019. PMID: 30321505 Review.
-
Risk estimations, risk factors, and genetic variants associated with Alzheimer's disease in selected publications from the Framingham Heart Study.J Alzheimers Dis. 2013;33 Suppl 1(0 1):S439-45. doi: 10.3233/JAD-2012-129040. J Alzheimers Dis. 2013. PMID: 22796871 Free PMC article. Review.
References
-
- Bernal J., Schreiber S., Menze I., Ostendorf A., Pfister M., Geisendorfer J., et al. (2023). Arterial hypertension and beta-amyloid accumulation have spatially overlapping effects on posterior white matter hyperintensity volume: A cross-sectional study. Alzheimers Res. Ther. 15:97. 10.1186/s13195-023-01243-4 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources