

Trends in Anterior Cruciate Ligament Reconstruction Techniques and Postoperative Care Among Leaders in the Field: A Survey of the Herodicus Society
- PMID: 39421046
- PMCID: PMC11483677
- DOI: 10.1177/23259671241274770
Trends in Anterior Cruciate Ligament Reconstruction Techniques and Postoperative Care Among Leaders in the Field: A Survey of the Herodicus Society
Abstract
Background: Despite a growing body of literature regarding anterior cruciate ligament reconstruction (ACLR), there remains a wide diversity in surgical technique and clinical practice across providers.
Purpose: To (1) describe current ACLR practice preferences among members of the Herodicus society and (2) determine whether these preferences are influenced by years in practice and overall surgical volume.
Study design: Cross-sectional study.
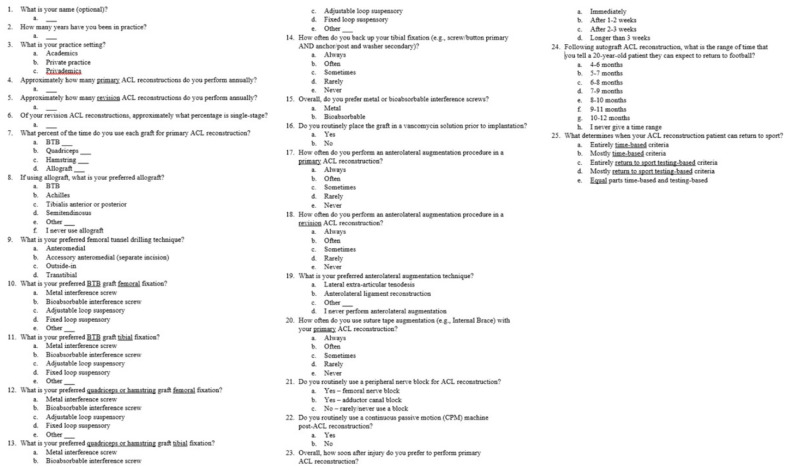
Methods: A 24-question survey investigating surgeons' practices and preferred ACLR surgical techniques was sent via email to all active Herodicus Society members. Survey responses were subdivided by years of experience and overall ACLR annual case volume. Descriptive statistics were compiled and chi-square testing was utilized to determine the significance of experience and case volume on survey responses.
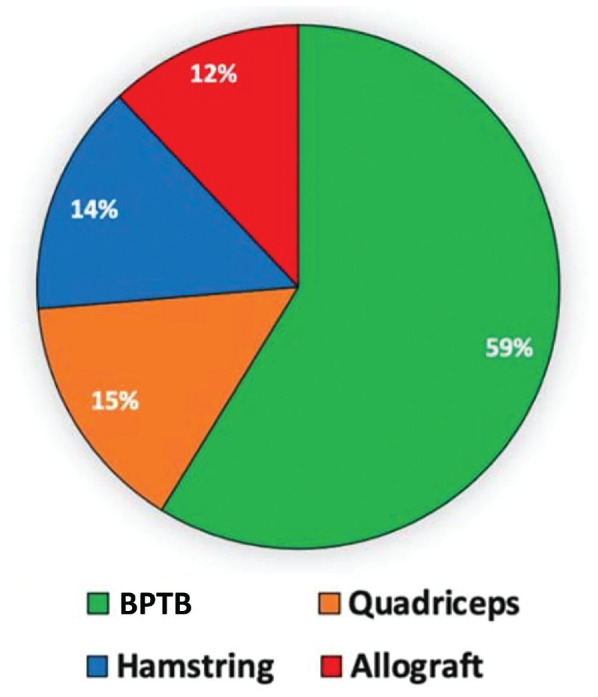
Results: Of the 113 invited Herodicus Society members who perform ACLR, 69 (61%) completed the survey. Respondents had a mean ± SD of 30.9 ± 9.8 years of experience in clinical practice and performed a mean of 96.0 ± 50.7 primary and 21.6 ± 16.9 revision ACLR annually. Of revision cases, 72.1% were performed using a single-stage technique. Mean frequency of graft usage by surgeon was bone-patellar tendon-bone autograft (58.6%), quadriceps autograft (14.6%), hamstring tendon autograft (14.0%), and allograft (11.8%). The plurality of surgeons responded that they used anterolateral augmentation "rarely" in primary ACLR (39.1%) and "sometimes" in revision ACLR (31.9%), with the majority performing lateral extra-articular tenodesis (66.7%) rather than anterolateral ligament reconstruction (14.5%). Most surgeons would not allow a 20-year-old football player to return before 7 months after ACLR (71.0%) but highly valued return-to-sports testing to determine readiness (94.2%). Higher volume surgeons performed single-stage revision ACLR at a significantly higher rate (79.8% vs 62.9%, P = .02) and significantly differed in return-to-sports criteria, with a greater proportion relying primarily on biometric testing (P = .01).
Conclusion: The survey demonstrated that, in the Herodicus Society, a wide range of preferences exist regarding ACLR surgical technique. Bone-patellar tendon-bone autograft is the most frequent primary ACLR graft choice. Most participants have not embraced newer techniques such as anterolateral or suture tape augmentation. Return to sports is generally not allowed before 7 months and heavily factors-in return-to-sports testing metrics, suggesting that purely time-based criteria for return to sports is not modern practice among elite sports medicine surgeons.
Keywords: ACL; ACLR; Herodicus Society; graft choice; knee ligaments.
© The Author(s) 2024.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: I.D.E. has received education payments from Arthrex, Mid-Atlantic Surgical Systems, Smith+Nephew; hospitality payments from Stryker; and a grant from Arthrex. M.A.F. has received education payments from Mid-Atlantic Surgical Systems. A.J.C. has received education payments from Arthrex, Medwest Associates, Mid-Atlantic Surgical Systems, Smith+Nephew, Supreme Orthopedic Systems; hospitality payments from Stryker; and a grant from Arthrex. J.W.A. has received education payments from Mid-Atlantic Surgical Systems; hospitality payments from Arthrex, Mid-Atlantic Surgical Systems, Smith+Nephew; and grants from Arthrex and DJO. V.M. has received nonconsulting fees from Smith & Nephew and Synthes GmbH; and consulting fees from Smith & Nephew. J.P.B. has received consulting fees from Arthrex and DJO; nonconsulting fees from Arthrex; royalties from Arthrex; and education payments from Fones Marketing Management. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Baron JE, Shamrock AG, Cates WT, et al.. Graft preparation with intraoperative vancomycin decreases infection after ACL reconstruction: a review of 1,640 cases. J Bone Joint Surg Am. 2019;101(24):2187-2193. - PubMed
-
- Beischer S, Gustavsson L, Senorski EH, et al.. Young athletes who return to sport before 9 months after anterior cruciate ligament reconstruction have a rate of new injury 7 times that of those who delay return. J Orthop Sports Phys Ther. 2020;50(2):83-90. - PubMed
-
- Budny J, Fox J, Rauh M, Fineberg M. Emerging trends in anterior cruciate ligament reconstruction. J Knee Surg. 2017;30(1):63-69. - PubMed
-
- Burgi CR, Peters S, Ardern CL, et al.. Which criteria are used to clear patients to return to sport after primary ACL reconstruction? A scoping review. Br J Sports Med. 2019;53(18):1154-1161. - PubMed
LinkOut - more resources
Full Text Sources
