

Three-Year Outcomes Following TAVR in Younger (<75 Years) Low-Surgical-Risk Severe Aortic Stenosis Patients
- PMID: 39421943
- PMCID: PMC11573113
- DOI: 10.1161/CIRCINTERVENTIONS.124.014018
Three-Year Outcomes Following TAVR in Younger (<75 Years) Low-Surgical-Risk Severe Aortic Stenosis Patients
Abstract
Background: Transcatheter aortic valve replacement (TAVR) is an alternative to surgery in patients with severe aortic stenosis, but data are limited on younger, low-risk patients. This analysis compares outcomes in low-surgical-risk patients aged <75 years receiving TAVR versus surgery.
Methods: The Evolut Low Risk Trial randomized 1414 low-risk patients to treatment with a supra-annular, self-expanding TAVR or surgery. We compared rates of all-cause mortality or disabling stroke, associated clinical outcomes, and bioprosthetic valve performance at 3 years between TAVR and surgery patients aged <75 years.
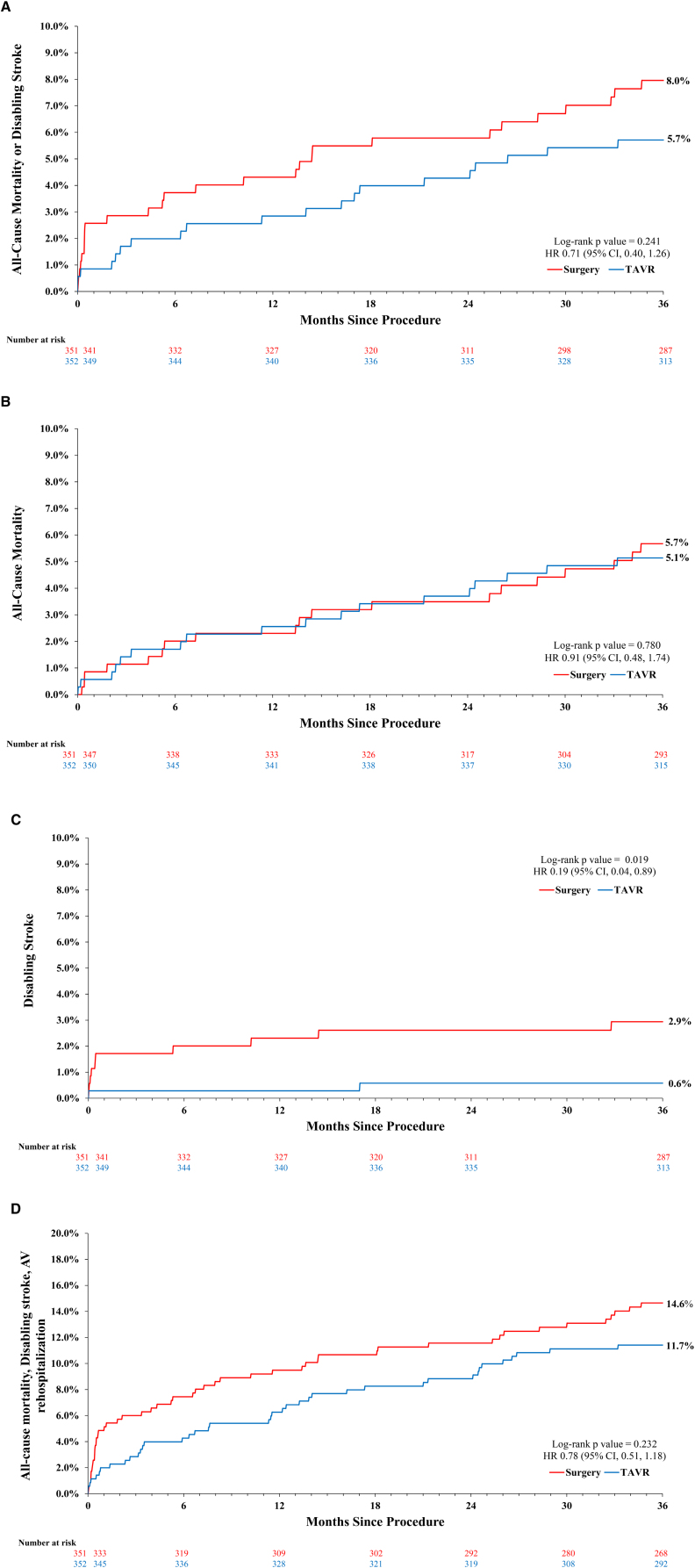
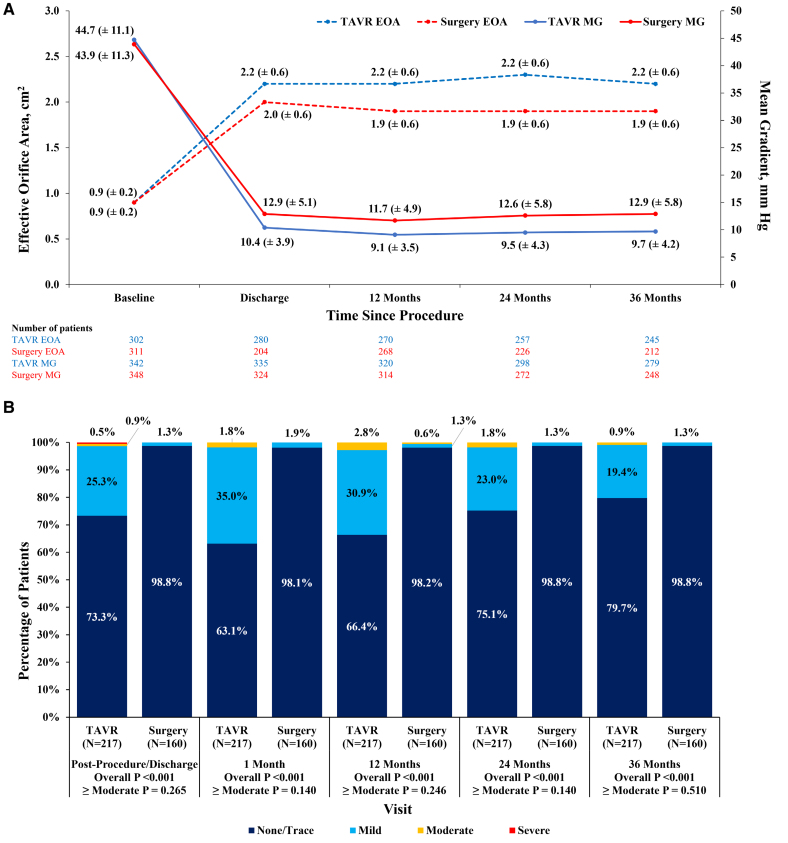
Results: In patients <75 years, 352 were randomized to TAVR and 351 to surgery. Mean age was 69.1±4.0 years (minimum 51 and maximum 74); Society of Thoracic Surgeons Predicted Risk of Mortality was 1.7±0.6%. At 3 years, all-cause mortality or disabling stroke for TAVR was 5.7% and 8.0% for surgery (P=0.241). Although there was no difference between TAVR and surgery in all-cause mortality, the incidence of disabling stroke was lower with TAVR (0.6%) than surgery (2.9%; P=0.019), while surgery was associated with a lower incidence of pacemaker implantation (7.1%) compared with TAVR (21.0%; P<0.001). Valve reintervention rates (TAVR 1.5%, surgery 1.5%, P=0.962) were low in both groups. Valve performance was significantly better with TAVR than surgery with lower mean aortic gradients (P<0.001) and lower rates of severe prosthesis-patient mismatch (P<0.001). Rates of valve thrombosis and endocarditis were similar between groups. There were no significant differences in rates of residual ≥moderate paravalvular regurgitation.
Conclusions: Low-risk patients <75 years treated with supra-annular, self-expanding TAVR had comparable 3-year all-cause mortality and lower disabling stroke compared with patients treated with surgery. There was significantly better valve performance in patients treated with TAVR.
Registration: URL: https://clinicaltrials.gov; Unique identifier: NCT02701283.
Keywords: aortic valve stenosis; humans; incidence; stroke; transcatheter aortic valve replacement.
Conflict of interest statement
Dr Modine is a consultant and Senior Advisory Board member for Medtronic. Dr Tchétché is a consultant for Medtronic. Dr Van Mieghem receives grants from Medtronic during the conduct of the trial and grants from Abbott Vascular, Edwards Lifesciences, Boston Scientific, Abiomed, PulseCath BV, and Daiichi Sankyo outside the submitted work. Dr Chetcuti receives personal fees from Medtronic; grants from Edwards, Boston Scientific, and Jena (paid to institution) during conduct of trial; and on an advisory board for Biotrace and Jena valve without remuneration. Dr Yakubov receives grants from Boston Scientific and Medtronic (paid to institution) and personal fees from Medtronic during the conduct of the trial. Dr Sorajja is a consultant to Boston Scientific and Medtronic. Dr Gada receives personal fees from Medtronic, Abbott Vascular, Becton Dickenson, and Boston Scientific outside the submitted work. Dr Mumtaz is a consultant and has received honoraria and research grants from Medtronic, Edwards, Atricure, Teleflex, Foldax, Japanese Organization for Medical Device Development, and Abbott. Dr Ramlawi receives grants, personal fees, and nonfinancial support from Medtronic, Liva Nova, and AtriCure. Dr Bajwa is a consultant for Medtronic. Dr Teirstein receives research grant and honoraria from Abbott, Boston Scientific, Cordis, and Medtronic, and serves on an advisory board for Boston Scientific and Medtronic. Dr Kleiman receives clinical trial reimbursement to his institution (Houston Methodist DeBakey Heart and Vascular Center) during the conduct of the trial. Dr Bagur serves as a consultant for Medtronic. Dr Chu receives Speakers’ honoraria from Medtronic, Edwards Lifesciences, Terumo Aortic and Artivion. Dr Huang is an employee and shareholder of Medtronic, plc. Dr Popma is a full-time employee and shareholder for Medtronic. Dr Forrest receives grant support/research contracts and consultant fees/honoraria/Speakers Bureau fees from Edwards Lifesciences and Medtronic. Dr Reardon receives grants from Medtronic (paid to institution) during conduct of trial, and consulting fees from Abbott, Boston Scientific, and Gore Medical (paid to institution) outside of the submitted work. The other authors report no conflicts.
Figures
References
-
- Popma JJ, Adams DH, Reardon MJ, Yakubov SJ, Kleiman NS, Heimansohn D, Hermiller J, Jr, Hughes GC, Harrison JK, Coselli J, et al. ; CoreValve United States Clinical Investigators. Transcatheter aortic valve replacement using a self-expanding bioprosthesis in patients with severe aortic stenosis at extreme risk for surgery. J Am Coll Cardiol. 2014;63:1972–1981. doi: 10.1016/j.jacc.2014.02.556 - PubMed
-
- Adams DH, Popma JJ, Reardon MJ, Yakubov SJ, Coselli JS, Deeb GM, Gleason TG, Buchbinder M, Hermiller J, Jr, Kleiman NS, et al. ; U.S. CoreValve Clinical Investigators. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370:1790–1798. doi: 10.1056/NEJMoa1400590 - PubMed
-
- Reardon MJ, Van Mieghem NM, Popma JJ, Kleiman NS, Søndergaard L, Mumtaz M, Adams DH, Deeb GM, Maini B, Gada H, et al. . Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2017;376:1321–1331. doi: 10.1056/NEJMoa1514616 - PubMed
-
- Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, et al. ; Evolut Low Risk Trial Investigators. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N Engl J Med. 2019;380:1706–1715. doi: 10.1056/NEJMoa1816885 - PubMed
-
- Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Pibarot P, et al. ; PARTNER 3 Investigators. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med. 2019;380:1695–1705. doi: 10.1056/NEJMoa1814052 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
