

The IMproving Preclinical Assessment of Cardioprotective Therapies (IMPACT): multicenter pig study on the effect of ischemic preconditioning
- PMID: 39422732
- PMCID: PMC11628588
- DOI: 10.1007/s00395-024-01083-9
The IMproving Preclinical Assessment of Cardioprotective Therapies (IMPACT): multicenter pig study on the effect of ischemic preconditioning
Abstract
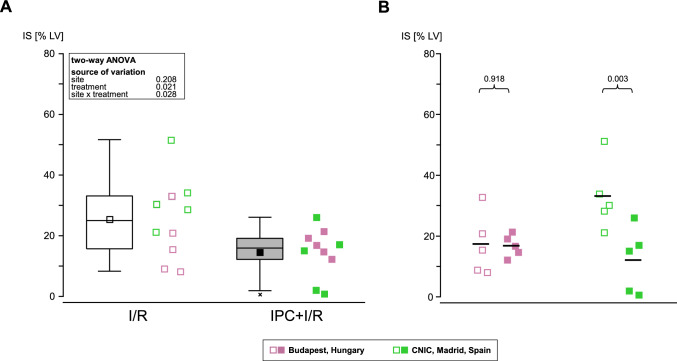
Numerous cardioprotective interventions have been reported to reduce myocardial infarct size (IS) in pre-clinical studies. However, their translation for the benefit of patients with acute myocardial infarction (AMI) has been largely disappointing. One reason for the lack of translation is the lack of rigor and reproducibility in pre-clinical studies. To address this, we have established the European IMproving Preclinical Assessment of Cardioprotective Therapies (IMPACT) pig AMI network with centralized randomization and blinded core laboratory IS analysis and validated the network with ischemic preconditioning (IPC) as a positive control. Ten sites in the COST Innovators Grant (IG16225) network participated in the IMPACT network. Three sites were excluded from the final analysis through quality control of infarct images and use of pre-defined exclusion criteria. Using a centrally generated randomization list, pigs were allocated to myocardial ischemia/reperfusion (I/R, N = 5/site) or IPC + I/R (N = 5/site). The primary endpoint was IS [% area-at-risk (AAR)], as quantified by triphenyl-tetrazolium-chloride (TTC) staining in a centralized, blinded core laboratory (5 sites), or IS [% left-ventricular mass (LV)], as quantified by a centralized, blinded cardiac magnetic resonance (CMR) core laboratory (2 sites). In pooled analyses, IPC significantly reduced IS when compared to I/R (57 ± 14 versus 32 ± 19 [%AAR] N = 25 pigs/group; p < 0.001; 25 ± 13 versus 14 ± 8 [%LV]; N = 10 pigs/group; p = 0.021). In site-specific analyses, in 4 of the 5 sites, IS was significantly reduced by IPC when compared to I/R when quantified by TTC and in 1 of 2 sites when quantified by CMR. A pig AMI multicenter European network with centralized randomization and core blinded IS analysis was established and validated with the aim to improve the reproducibility of cardioprotective interventions in pre-clinical studies and the translation of cardioprotection for patient benefit.
Keywords: Acute myocardial infarction; Ischemia/reperfusion injury; Ischemic preconditioning; Multicenter network; Pig; Randomized-controlled trial.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: P.F. is the founder and CEO and ZG is involved in the management of Pharmahungary Group, a group of R&D companies. Pharmahungary Group has a conflict of interest as it may be organizing multicenter studies on cardioprotection on external request and potentially including the here validated sites of the current COST action (IG16225). D.J.H. has received: consultant fees from Faraday Pharmaceuticals Inc. and Boehringer Ingelheim International GmbH; honoraria from Servier; and research funding from Astra Zeneca, Merck Sharp & Dohme Corp and Novonordisk. J. L. Z. received speaker honoraria from Pfizer, Bayer, Novartis, and Amgem. All other authors declare no competing interests. Ethical statements: The experimental protocols conformed to the EU directive 2010/63EU on the protection of animals used for scientific purposes and the Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines [49]. The experimental protocols were formally approved by the appropriate national or institutional ethics committees (see Suppl. Data sheet experimental design).
Figures





Comment in
-
CAESAR lives on with IMPACT: bringing rigor and relevance to cardioprotection research.Basic Res Cardiol. 2024 Dec;119(6):889-892. doi: 10.1007/s00395-024-01082-w. Epub 2024 Oct 18. Basic Res Cardiol. 2024. PMID: 39422733 No abstract available.
References
-
- Alburquerque-Bejar JJ, Barba I, Inserte J, Miro-Casas E, Ruiz-Meana M, Poncelas M, Vilardosa U, Valls-Lacalle L, Rodriguez-Sinovas A, Garcia-Dorado D (2015) Combination therapy with remote ischaemic conditioning and insulin or exenatide enhances infarct size limitation in pigs. Cardiovasc Res 107:246–254. 10.1093/cvr/cvv171 - PubMed
-
- Baranyai T, Giricz Z, Varga ZV, Koncsos G, Lukovic D, Makkos A, Sarkozy M, Pavo N, Jakab A, Czimbalmos C, Vago H, Ruzsa Z, Toth L, Garamvolgyi R, Merkely B, Schulz R, Gyongyosi M, Ferdinandy P (2017) In vivo MRI and ex vivo histological assessment of the cardioprotection induced by ischemic preconditioning, postconditioning and remote conditioning in a closed-chest porcine model of reperfused acute myocardial infarction: importance of microvasculature. J Transl Med 15:67. 10.1186/s12967-017-1166-z - PMC - PubMed
-
- Blöndal M, Ainla T, Eha J, Löiveke P, Marandi T, Saar A, Veldre G, Edfors R, Lewinter C, Jernberg T, Jortveit J, Halvorsen S, Becker D, Csanadi Z, Ferenci T, Andreka P, Janosi A (2022) Comparison of management and outcomes of ST-segment elevation myocardial infarction patients in Estonia, Hungary, Norway, and Sweden according to national ongoing registries. Eur Heart J Qual Care Clin Outcomes 8:307–314. 10.1093/ehjqcco/qcaa098 - PubMed
Publication types
MeSH terms
Grants and funding
- grant CEX2020-001041-S funded by MICIN/AEI/10.13039/501100011033/Severo Ochoa Center of Excellence
- Singapore Translational Research Investigator Award (MOH-STaR21jun-0003)MOH-STaR21jun-0003/Duke-NUS Signature Research Programme
- Centre Grant scheme (NMRC CG21APR1006)/Duke-NUS Signature Research Programme
- Collaborative Centre Grant scheme (NMRC/CG21APRC006)/Duke-NUS Signature Research Programme
- 2020-1.1.5-GYORSÍTÓSÁV-2021-00011/Ministry for Innovation and Technology in Hungary
- RRF-2.3.1-21-2022-00003 "National Heart Laboratory/Ministry for Innovation and Technology in Hungary
- Hungary"/Ministry for Innovation and Technology in Hungary
- OTKA-138223/Hungarian National Scientific Research Fund
- ISCIII/Instituto de Salud Carlos III
- grant PI20/0247/Instituto de Salud Carlos III
- Centro Nacional de Investigaciones Cardiovasculares
- Ministerio de Ciencia e Innovación
- Pro CNIC Foundation
- CRC 1116 B8/Deutsche Forschungsgemeinschaft
- RTG 2989/Deutsche Forschungsgemeinschaft
- CA 22169/European Union COST Action METAHEART
- CARREM/Ludwig Boltzmann Gesellschaft
LinkOut - more resources
Full Text Sources
Medical
