

Assessment of trabecular bone score using updated TBSTT in anorexia nervosa-The AN-BO study
- PMID: 39423193
- PMCID: PMC11488700
- DOI: 10.1371/journal.pone.0311499
Assessment of trabecular bone score using updated TBSTT in anorexia nervosa-The AN-BO study
Abstract
Objective: Anorexia Nervosa (AN) is characterized by a distortion of body image, very low body weight, malnutrition and hormonal dysregulations, resulting in reduced bone mineral density (BMD) and impaired bone microarchitecture. The updated Trabecular Bone Score (TBS) algorithm accounts for soft tissue thickness (TBSTT) instead of BMI (TBSBMI). The aim of the study was to assess both TBS algorithms in adult AN patients compared to normal-weight controls(CTRL).
Method: This retrospective cross-sectional study investigated 34 adult female anorexia nervosa (AN) patients and 26 healthy normal-weighted age- and sex-matched controls (CTRL). Bone texture analysis was assessed by TBSTT and TBSBMI (TBS iNsight® V4.0 and V3.1), bone mineral density (BMD; lumbar spine LS, femoral neck, total hip) and body composition by DXA (GE Lunar iDXATM). Laboratory analyses included bone turnover markers (CTX; P1NP; sclerostin). Data analysis was performed using parametric (t-test) or non-parametric test (Mann-Whitney-U-Test) depending on normality, one-way ANCOVA and correlation analysis (Perason's or Spearman's).
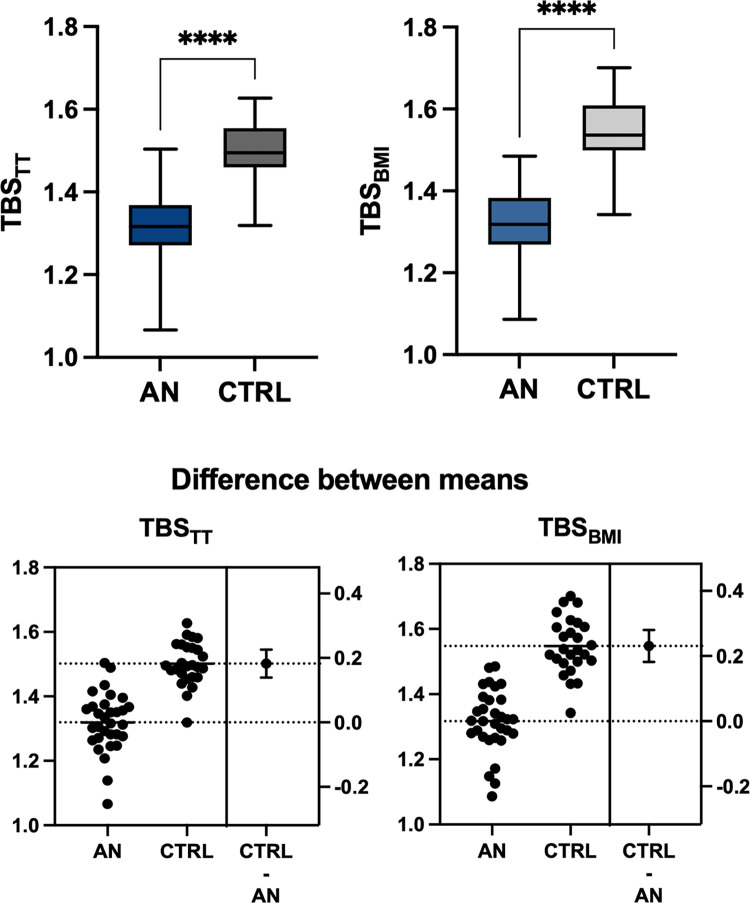
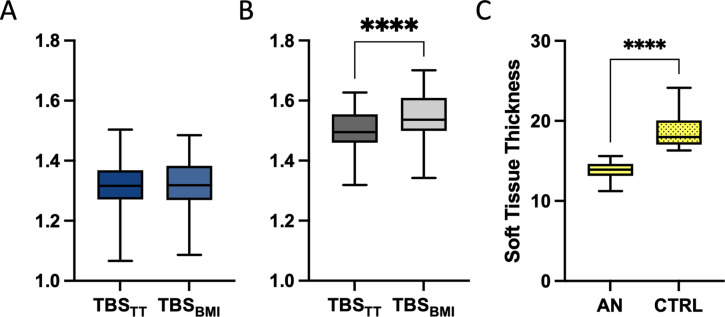
Results: AN patients (BMI 14.7(1.6)) and CTRL (BMI 22.4(4.0)) were of comparable age (22.8(7.1) vs.25.0(4.0)years, p = 0.145). TBSTT(1.319±0.09 vs.1.502±0.07, p<0.001) and TBSBMI(1.317±0.10 vs.1.548±0.09, p<0.001) were significantly lower in AN patients compared to CTRL. Soft tissue thickness was lower in AN (p<0.001). Within the CTRL group, but not in AN, TBSTT and TBSBMI were significantly different (p<0.001). BMD was lower at all sites in AN patients (p<0.001 for all), being lowest at LS. Bone Mineral Content, Lean Body mass and Fat Mass were lower in AN (p<0.001). AN patients had lower P1NP (p = 0.05), but higher CTX (p = 0.001) and sclerostin (p = 0.003) levels.
Conclusion: Adult AN patients have lower TBSTT and TBSBMI, reduced BMD and an uncoupling of bone turnover. In AN both TBS algorithms show similar reduced trabecular bone microarchitecture. The observed difference of TBSTT and TBSBMI in CTRL with normal body composition highlight the importance of the new algorithm.
Copyright: © 2024 Haschka et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Didier Hans is co-owner of the TBS patent and has corresponding ownership shares and position at Medimaps group.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
