

Predictors of response to CDK4/6i retrial after prior CDK4/6i failure in ER+ metastatic breast cancer
- PMID: 39424631
- PMCID: PMC11489574
- DOI: 10.1038/s41523-024-00699-3
Predictors of response to CDK4/6i retrial after prior CDK4/6i failure in ER+ metastatic breast cancer
Abstract
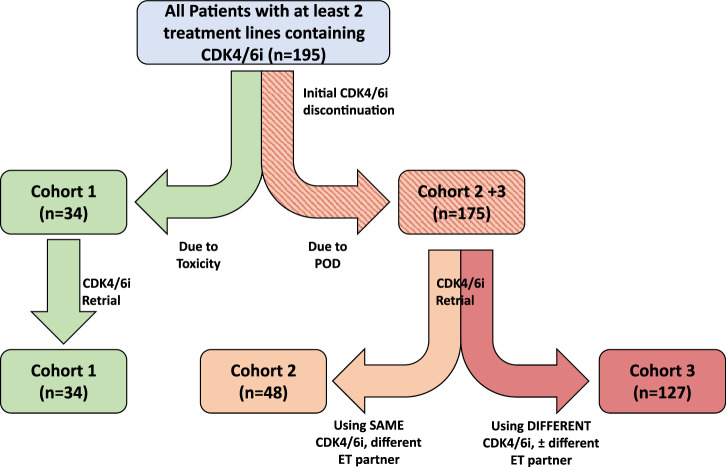
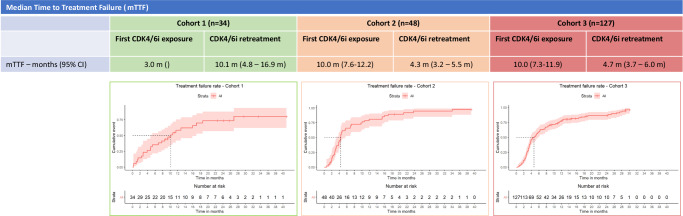
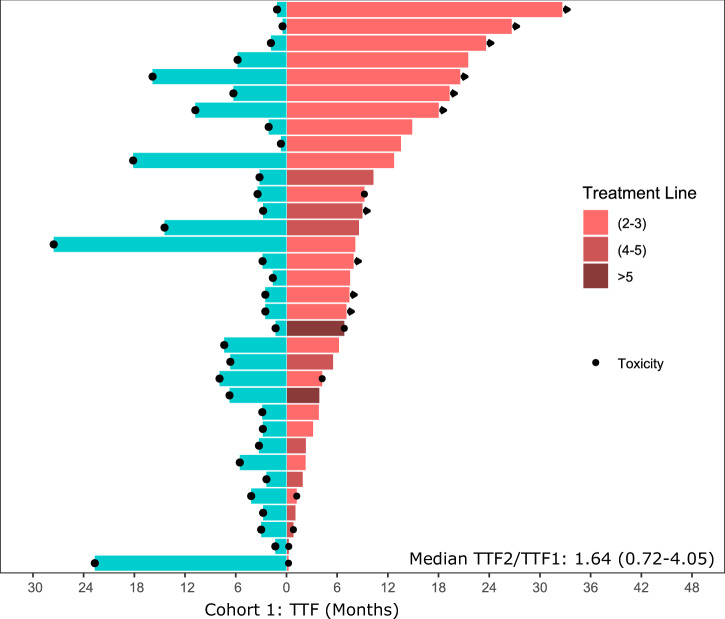
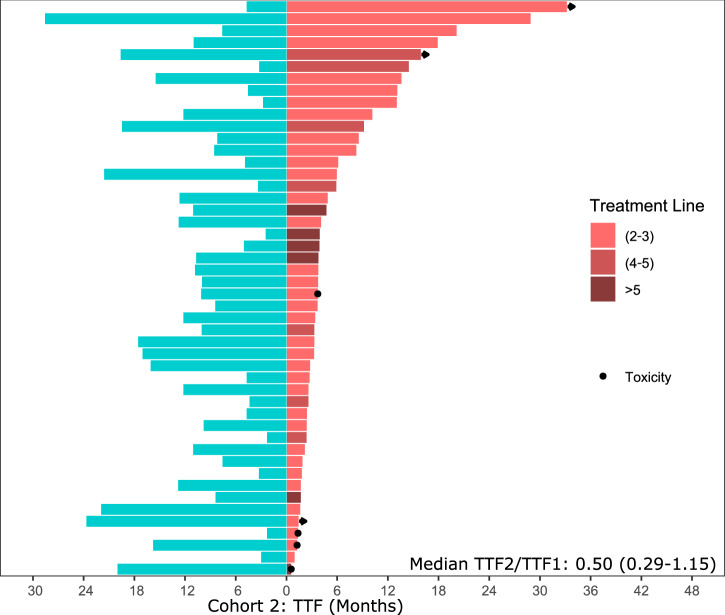
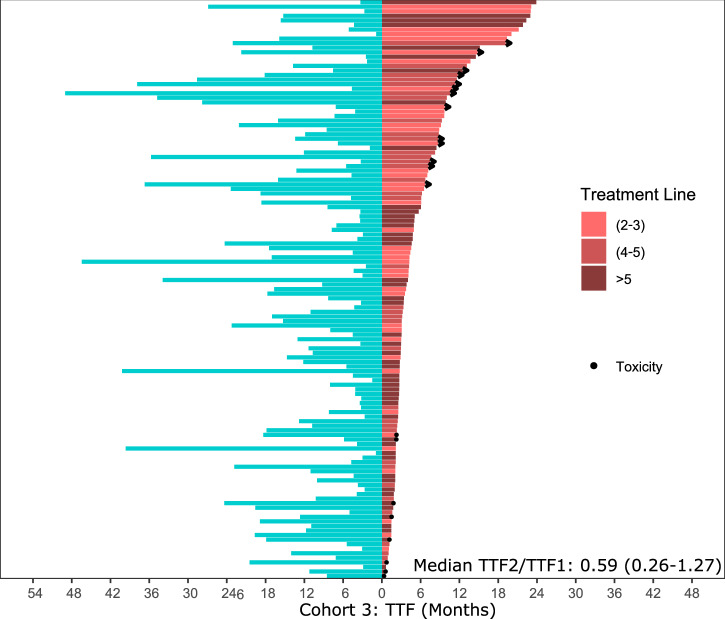
After disease progression on endocrine therapy (ET) plus a CDK4/6 inhibitor, there is no standardized sequence for subsequent treatment lines for estrogen receptor positive (ER+) metastatic breast cancer (MBC). CDK4/6i retrial as a treatment strategy is commonplace in modern clinical practice; however, the available prospective data investigating this strategy have had inconclusive results. To frame this data in a real-world context, we performed a retrospective analysis assessing the efficacy of CDK4/6is in 195 patients who had previous exposure to CDK4/6i in a prior treatment line at our institution. Among patients who had stopped a CDK4/6i due to toxicity, CDK4/6i retrial either immediately after with a different CDK4/6i or in a further treatment line with the same initial CDK4/6i was both safe and effective, with a median time to treatment failure (TTF) of 10.1 months (95%CI, 4.8-16.9). For patients whose disease progressed on a prior CDK4/6i, we demonstrated comparable median TTFs for patients rechallenged with the same CDK4/6i (4.3 months, 95%CI 3.2-5.5) and with a different CDK4/6i (4.7 months, 95%CI 3.7-6.0) when compared to the recent PACE, PALMIRA, and MAINTAIN trials. Exploratory genomic analysis suggested that the presence of mutations known to confer CDK4/6i resistance, such as TP53 mutations, CDK4 amplifications, and RB1 or FAT1 loss of function mutations may be molecular biomarkers predictive of CDK4/6i retrial failure.
© 2024. The Author(s).
Conflict of interest statement
Larry Norton, MD is the Editor-in-Chief for
Figures

Update of
-
Predictors of Response to CDK4/6i Retrial After Prior CDK4/6i Failure in ER+ Metastatic Breast Cancer.Res Sq [Preprint]. 2024 May 2:rs.3.rs-4237867. doi: 10.21203/rs.3.rs-4237867/v1. Res Sq. 2024. Update in: NPJ Breast Cancer. 2024 Oct 18;10(1):92. doi: 10.1038/s41523-024-00699-3. PMID: 38746324 Free PMC article. Updated. Preprint.
References
-
- Noone AMHN et al. Cancer Statistics Review, 1975-2018 - SEER Statistics. https://seer.cancer.gov/archive/csr/1975_2018/ (2018).
-
- Goyal, R. K. et al. Overall survival associated with CDK4/6 inhibitors in patients with HR+/HER2– metastatic breast cancer in the United States: a SEER-Medicare population-based study. Cancer129, 1051–1063 (2023). - PubMed
-
- Im, S.-A. et al. Overall survival with ribociclib plus endocrine therapy in breast cancer. N. Engl. J. Med.381, 307–316 (2019). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
