

A time series algorithm to predict surgery in neonatal necrotizing enterocolitis
- PMID: 39425161
- PMCID: PMC11487704
- DOI: 10.1186/s12911-024-02695-w
A time series algorithm to predict surgery in neonatal necrotizing enterocolitis
Abstract
Background: Determining the optimal timing of surgical intervention for Neonatal necrotizing enterocolitis (NEC) poses significant challenges. This study develops a predictive model using the long short-term memory network (LSTM) with a focal loss (FL) to identify infants at risk of developing Bell IIB + NEC early and issue timely surgical warnings.
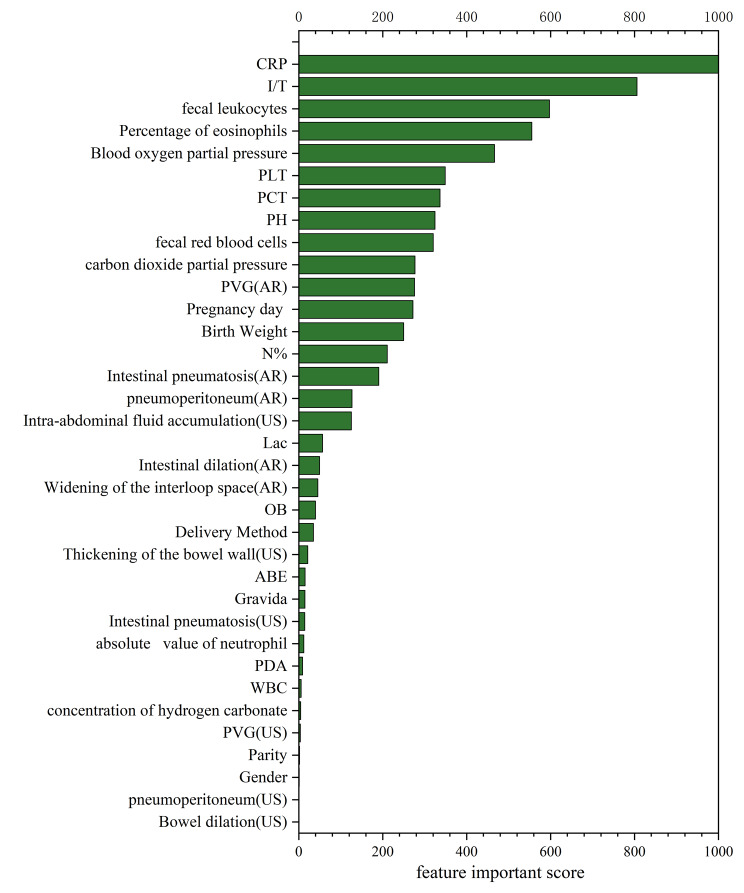
Methods: Data from 791 neonates diagnosed with NEC are gathered from the Neonatal Intensive Care Unit (NICU), encompassing 35 selected features. Infants are categorized into those requiring surgical intervention (n = 257) and those managed medically (n = 534) based on the Mod-Bell criteria. A fivefold cross-validation approach is employed for training and testing. The LSTM algorithm is utilized to capture and utilize temporal relationships in the dataset, with FL employed as a loss function to address class imbalance. Model performance metrics include precision, recall, F1 score, and average precision (AP).
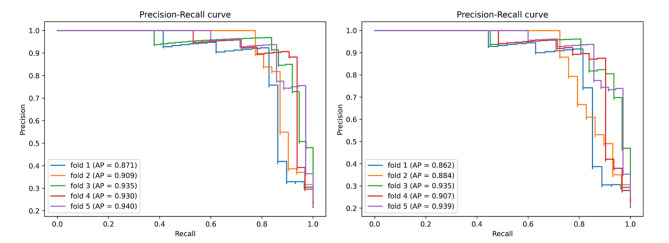
Results: The model tested on a real dataset demonstrated high performance. Predicting surgical risk 1 day in advance achieved precision (0.913 ± 0.034), recall (0.841 ± 0.053), F1 score (0.874 ± 0.029), and AP (0.917 ± 0.025). The 2-days-in-advance predictions yielded (0.905 ± 0.036), recall (0.815 ± 0.057), F1 score (0.857 ± 0.035), and AP (0.905 ± 0.029).
Conclusion: The LSTM model with FL exhibits high precision and recall in forecasting the need for surgical intervention 1 or 2 days ahead. This predictive capability holds promise for enhancing infants' outcomes by facilitating timely clinical decisions.
Keywords: Auxiliary diagnosis; Deep learning; Long short-term memory network; Neonatal necrotizing enterocolitis; Predictive surgery.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures








References
-
- Hein-Nielsen AL, Petersen SM, Greisen G. Unchanged incidence of necrotising enterocolitis in a tertiary neonatal department. Dan Med J. 2015;62:A5091. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
