

Therapeutic potential of agents targeting cannabinoid type 2 receptors in organ fibrosis
- PMID: 39425446
- PMCID: PMC11489134
- DOI: 10.1002/prp2.1219
Therapeutic potential of agents targeting cannabinoid type 2 receptors in organ fibrosis
Abstract
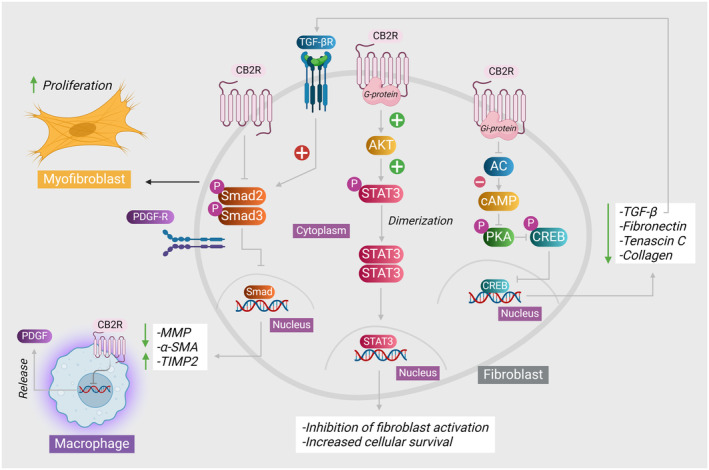
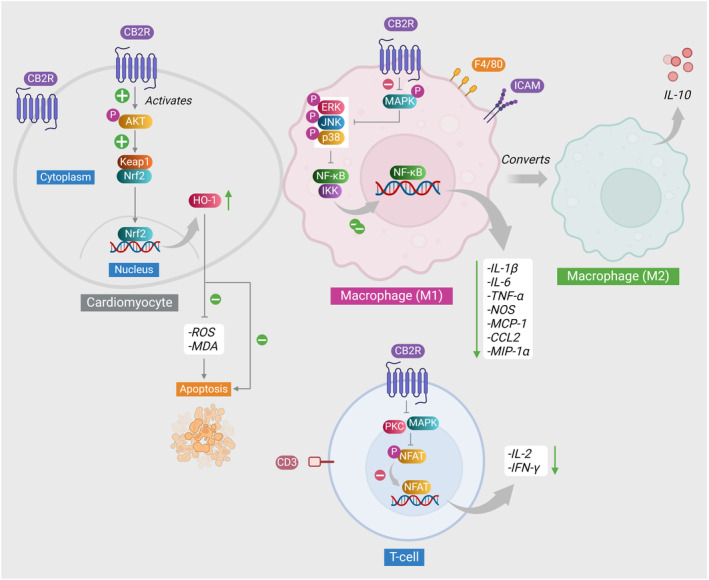
The endocannabinoid system has garnered attention as a potential therapeutic target in a range of pathological disorders. Cannabinoid receptors type 2 (CB2) are a class of G protein-coupled receptors responsible for transmitting intracellular signals triggered by both endogenous and exogenous cannabinoids, including those derived from plants (phytocannabinoids) or manufactured synthetically (synthetic cannabinoids). Recent recognition of the role of CB2 receptors in fibrosis has fueled interest in therapeutic targeting of CB2 receptors in fibrosis. Fibrosis is characterized by the alteration of the typical cellular composition within the tissue parenchyma, resulting from exposure to diverse etiological factors. The pivotal function of CB2 agonists has been widely recognized in the regulation of inflammation, fibrogenesis, and various other biological pathologies. The modulation of CB2 receptors, whether by enhancing their expression or activating their function, has the potential to provide benefits in numerous conditions, particularly by avoiding any associated adverse effects on the central nervous system. The sufficient activation of CB2 receptors resulted in the complete suppression of gene expression related to transforming growth factor β1 and its subsequent fibrogenic response. Multiple reports have also indicated the diverse functions that CB2 agonists possess in mitigating chronic inflammation and subsequent fibrosis development in various types of tissues. While currently in the preclinical stage, the advancement of CB2 compounds has garnered significant attention within the realm of drug discovery. This review presents a comprehensive synthesis of various independent experimental studies elucidating the pivotal role of identified natural and synthetic CB2 agonists in the pathophysiology of organ fibrosis, specifically in the cardiac, hepatic, and renal systems.
Keywords: CB2 agonists; cannabinoids; cardiac fibrosis; fibrosis; phytocannabinoids; renal fibrosis.
© 2024 The Author(s). Pharmacology Research & Perspectives published by British Pharmacological Society and American Society for Pharmacology and Experimental Therapeutics and John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
