

Preoperative prediction of diffuse glioma type and grade in adults: a gadolinium-free MRI-based decision tree
- PMID: 39425768
- PMCID: PMC11836213
- DOI: 10.1007/s00330-024-11140-5
Preoperative prediction of diffuse glioma type and grade in adults: a gadolinium-free MRI-based decision tree
Abstract
Objectives: To develop a gadolinium-free MRI-based diagnosis prediction decision tree (DPDT) for adult-type diffuse gliomas and to assess the added value of gadolinium-based contrast agent (GBCA) enhanced images.
Materials and methods: This study included preoperative grade 2-4 adult-type diffuse gliomas (World Health Organization 2021) scanned between 2010 and 2021. The DPDT, incorporating eleven GBCA-free MRI features, was developed using 18% of the dataset based on consensus readings. Diagnosis predictions involved grade (grade 2 vs. grade 3/4) and molecular status (isocitrate dehydrogenase (IDH) and 1p/19q). GBCA-free diagnosis was predicted using DPDT, while GBCA-enhanced diagnosis included post-contrast images. The accuracy of these predictions was assessed by three raters with varying experience levels in neuroradiology using the test dataset. Agreement analyses were applied to evaluate the prediction performance/reproducibility.
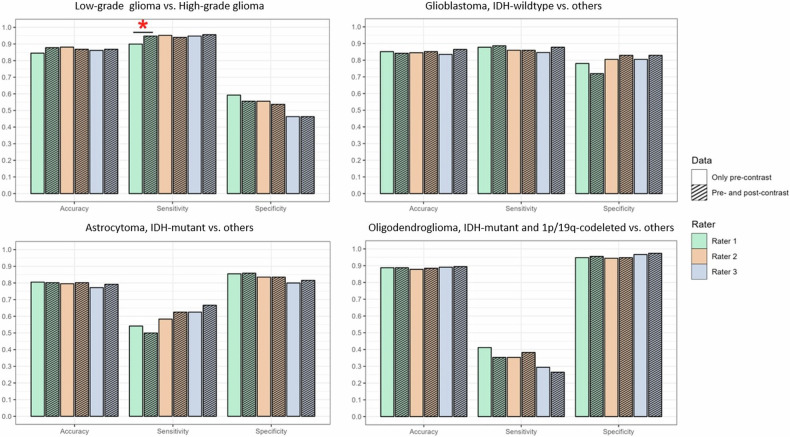
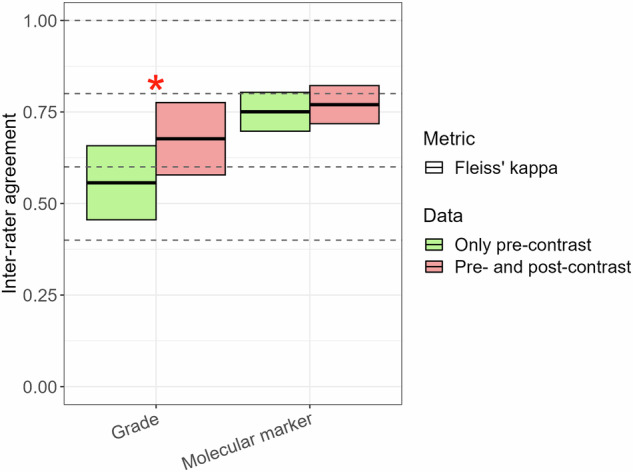
Results: The test dataset included 303 patients (age (SD): 56.7 (14.2) years, female/male: 114/189, low-grade/high-grade: 54/249, IDH-mutant/wildtype: 82/221, 1p/19q-codeleted/intact: 34/269). Per-rater GBCA-free predictions achieved ≥ 0.85 (95%-CI: 0.80-0.88) accuracy for grade and ≥ 0.75 (95%-CI: 0.70-0.80) for molecular status, while GBCA-enhanced predictions reached ≥ 0.87 (95%-CI: 0.82-0.90) and ≥ 0.77 (95%-CI: 0.71-0.81), respectively. No accuracy difference was observed between GBCA-free and GBCA-enhanced predictions. Group inter-rater agreement was moderate for GBCA-free (0.56 (95%-CI: 0.46-0.66)) and substantial for GBCA-enhanced grade prediction (0.68 (95%-CI: 0.58-0.78), p = 0.008), while substantial for both GBCA-free (0.75 (95%-CI: 0.69-0.80) and GBCA-enhanced (0.77 (95%-CI: 0.71-0.82), p = 0.51) molecular status predictions.
Conclusion: The proposed GBCA-free diagnosis prediction decision tree performed well, with GBCA-enhanced images adding little to the preoperative diagnostic accuracy of adult-type diffuse gliomas.
Key points: Question Given health and environmental concerns, is there a gadolinium-free imaging protocol to preoperatively evaluate gliomas comparable to the gadolinium-enhanced standard practice? Findings The proposed gadolinium-free diagnosis prediction decision tree for adult-type diffuse gliomas performed well, and gadolinium-enhanced MRI demonstrated only limited improvement in diagnostic accuracy. Clinical relevance Even inexperienced raters effectively classified adult-type diffuse gliomas using the gadolinium-free diagnosis prediction decision tree, which, until further validation, can be used alongside gadolinium-enhanced images to respect standard practice, despite this study showing that gadolinium-enhanced images hardly improved diagnostic accuracy.
Keywords: Brain neoplasms; Gadolinium; Glioma; Isocitrate dehydrogenase; Magnetic resonance imaging.
© 2024. The Author(s).
Conflict of interest statement
Compliance with ethical standards. Guarantor: The scientific guarantor of this publication is Vera C. Keil. Conflict of interest: The authors of this manuscript declare relationships with the following companies: V.C.K.: Lilly Pharma (Consulting); Junior Deputy Editor for European Radiology, as such they did not participate in the selection or review processes for this article. The remaining authors declare no conflicts of interest. Statistics and biometry: One of the authors has significant statistical expertise. Informed consent: Written informed consent was waived by the Institutional Review Board. Ethical approval: Institutional Review Board approval was obtained. Study subjects or cohorts overlap: The same study cohort was used in another study, which was recently accepted by the Journal of Neuroimaging on August 14, 2024. The in-press study explored a different research question focused on predicting glioma enhancement features using the proposed Enhancement Prediction Decision Tree. Methodology: Retrospective Observational Performed at one institution
Figures


References
-
- Castet F, Alanya E, Vidal N et al (2019) Contrast-enhancement in supratentorial low-grade gliomas: a classic prognostic factor in the molecular age. J Neurooncol 143:515–523 - PubMed
-
- Eichberg DG, Di L, Morell AA et al (2020) Incidence of high grade gliomas presenting as radiographically non-enhancing lesions: experience in 111 surgically treated non-enhancing gliomas with tissue diagnosis. J Neurooncol 147:671–679 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
