

Treatment of mild to moderate community-acquired pneumonia in previously healthy children: an Italian intersociety consensus (SIPPS-SIP-SITIP-FIMP-SIAIP-SIMRI-FIMMG-SIMG)
- PMID: 39427174
- PMCID: PMC11491012
- DOI: 10.1186/s13052-024-01786-8
Treatment of mild to moderate community-acquired pneumonia in previously healthy children: an Italian intersociety consensus (SIPPS-SIP-SITIP-FIMP-SIAIP-SIMRI-FIMMG-SIMG)
Abstract
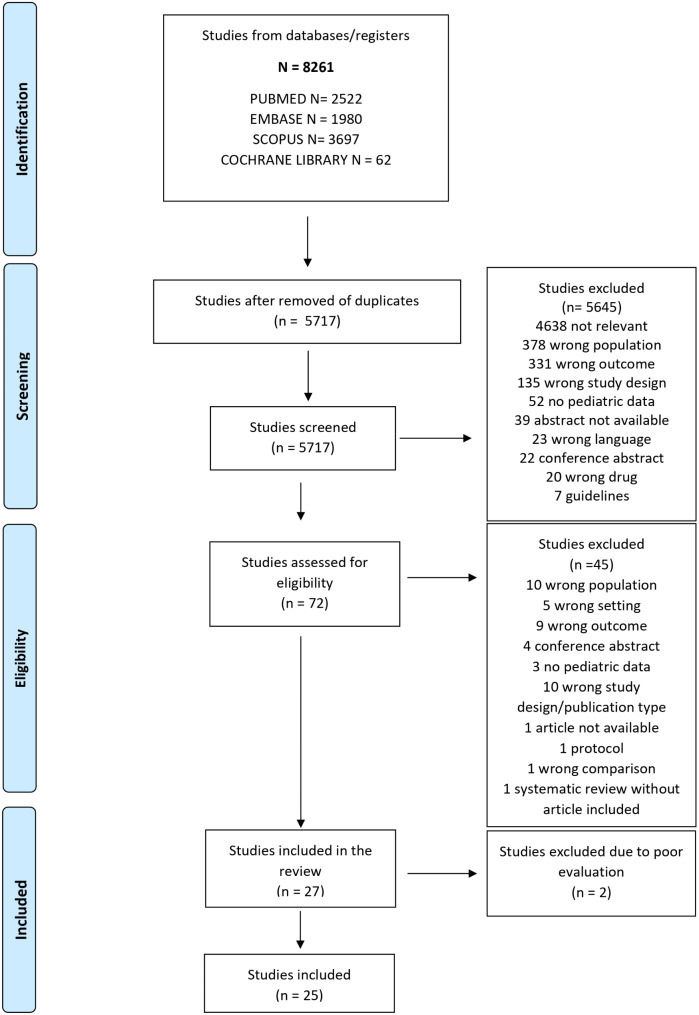
Community-acquired pneumonia (CAP) is an acute infection of the lung parenchyma acquired outside the hospital or other healthcare settings, typically affecting previously healthy individuals. This intersociety consensus aims to provide evidence-based recommendations for the antibiotic treatment of mild to moderate CAP in previously healthy children in Italy.A systematic review was conducted to identify the most recent and relevant evidence. Embase, Scopus, PubMed, and Cochrane databases were systematically screened, with a date restriction from 2012 to April 2024, but without language limitations. The review included studies conducted in high-income countries on antibiotic therapy in children over 3 months of age diagnosed with mild-moderate CAP. The certainty of evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methods. The final recommendations were obtained through a Delphi consensus of an expert panel.Amoxicillin is the first-line treatment if the child is at least immunized against Haemophilus influenzae type b (low/very low quality of evidence, strong recommendations), while amoxicillin-clavulanate or second- or third-generation cephalosporins should be prescribed for those unimmunized or with incomplete immunization coverage for both H. influenzae type b and Streptococcus pneumoniae (low/very low quality of evidence, strong recommendations). Macrolides should be considered in addition to amoxicillin in children over 5 years old, if symptoms persist and the clinical condition remains good after 48 h of therapy (low/very low quality of evidence, strong recommendations). The dosage of amoxicillin is 90 mg/kg/day divided in three doses, although two doses could be considered to improve compliance (moderate quality of evidence, weak recommendations). A five-day duration of therapy is recommended, with clinical monitoring and re-assessment approximately 72 h after the start of antibiotic treatment to evaluate symptom resolution (moderate quality of evidence, strong recommendations).To improve the management of CAP in pediatric patients, we have developed this consensus based on a thorough review of the best available evidence and extensive discussions with an expert panel. However, further efforts are needed. Future research should focus on enhancing diagnostic accuracy, optimizing antibiotic utilization, comparing the efficacy of different antibiotic regimens, and determining the optimal dosage and duration of treatment in different setting.
Keywords: Antibiotic therapy; Community-acquired pneumonia; Pediatric infectious diseases; Primary care; Respiratory infections.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Liu L, Johnson H, Cousens S, Perin J, Scott S, Lawn J, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;9832:2151–61. - PubMed
-
- Zar H, Ferkol T. The global burden of respiratory disease-impact on child health. Pediatr Pulmonol. 2014;49(5):430–4. - PubMed
-
- WHO. World Health Statistics. World Health Organization. 2015. https://www.who.int/docs/default-source/gho-documents/world-health-stati.... 2015;available.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
