

CHF6523 data suggest that the phosphoinositide 3-kinase delta isoform is not a suitable target for the management of COPD
- PMID: 39427187
- PMCID: PMC11491004
- DOI: 10.1186/s12931-024-02999-5
CHF6523 data suggest that the phosphoinositide 3-kinase delta isoform is not a suitable target for the management of COPD
Abstract
Background: Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory condition. Given patients with COPD continue to experience exacerbations despite the availability of effective therapies, anti-inflammatory treatments targeting novel pathways are needed. Kinases, notably the phosphoinositide 3-kinases (PI3K), are thought to be involved in chronic airway inflammation, with this pathway proposed as a critical regulator of inflammation and oxidative stress response in COPD. CHF6523 is an inhaled PI3Kδ inhibitor that has shown positive preclinical results. This manuscript reports the results of a study of CHF6523 in patients with stable COPD (chronic bronchitis phenotype), and who had evidence of type-2 inflammation.
Methods: This randomised, double-blind, placebo-controlled, two-way crossover study comprised two 28-day treatment periods separated by a 28-day washout. Patients (N = 44) inhaled CHF6523 in one period, and placebo in the other, both twice daily. The primary objective was to assess the safety and tolerability of CHF6523; the secondary objective was to assess CHF6523 pharmacokinetics. Exploratory endpoints included target engagement (the relative reduction in phosphatidylinositol (3,4,5)-trisphosphate [PIP3]), pharmacodynamic evaluations such as airflow obstruction, and hyperinflation, and to identify biomarker(s) of drug response using proteomics and transcriptomics.
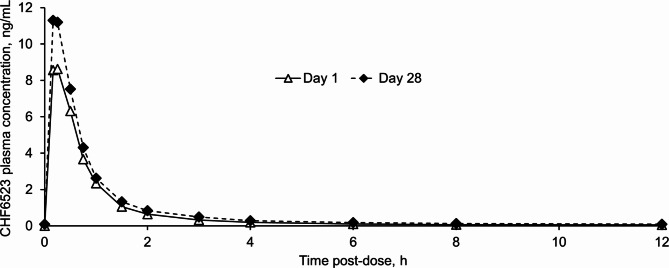
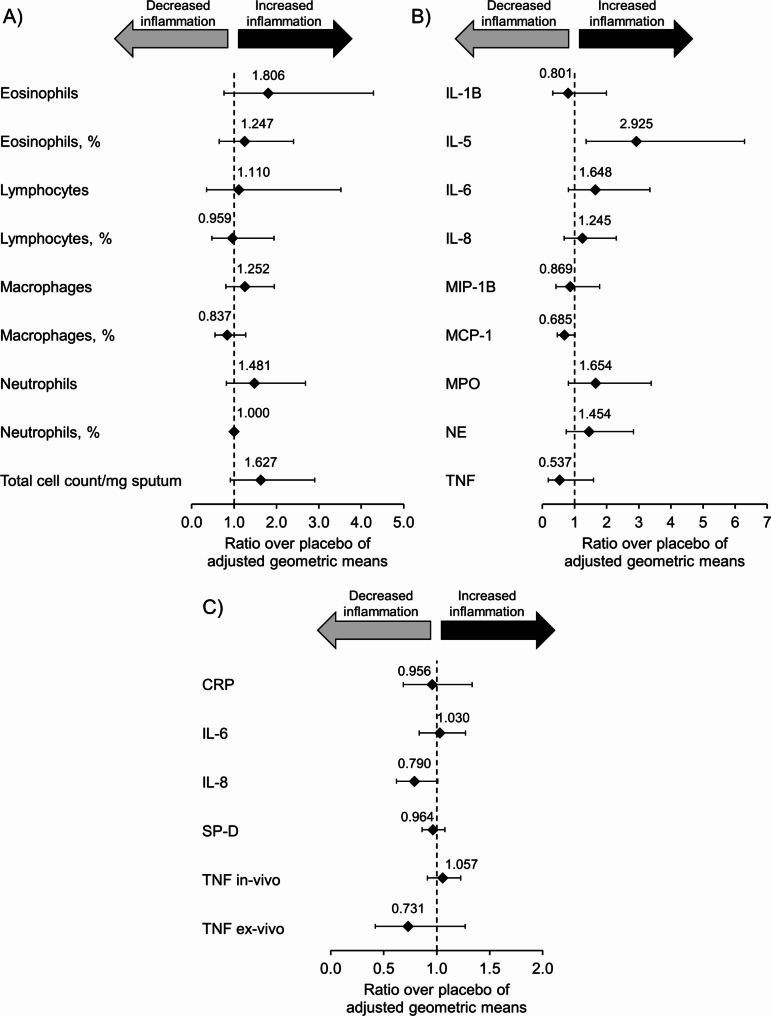
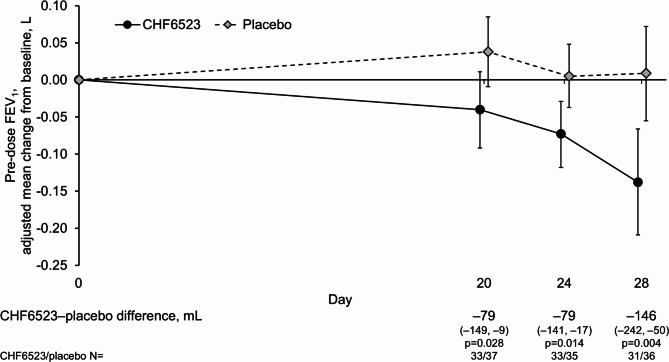
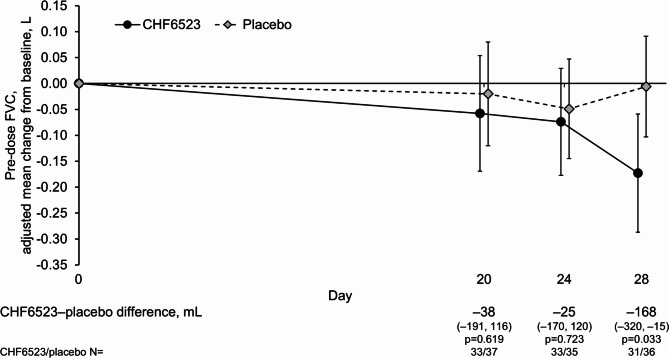
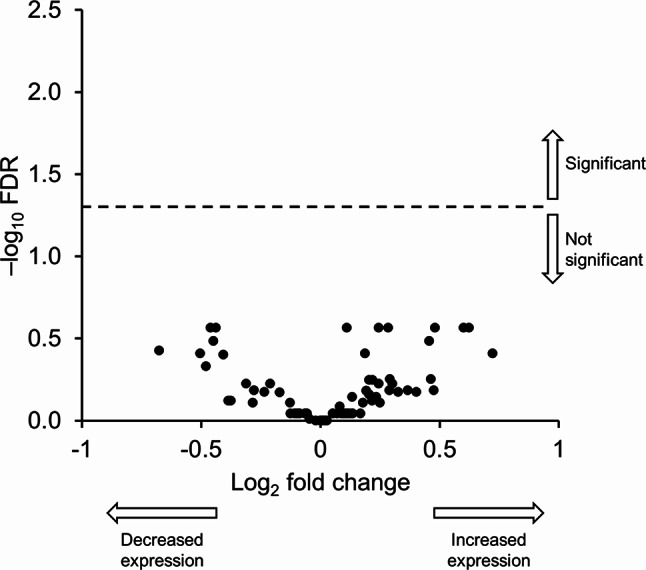
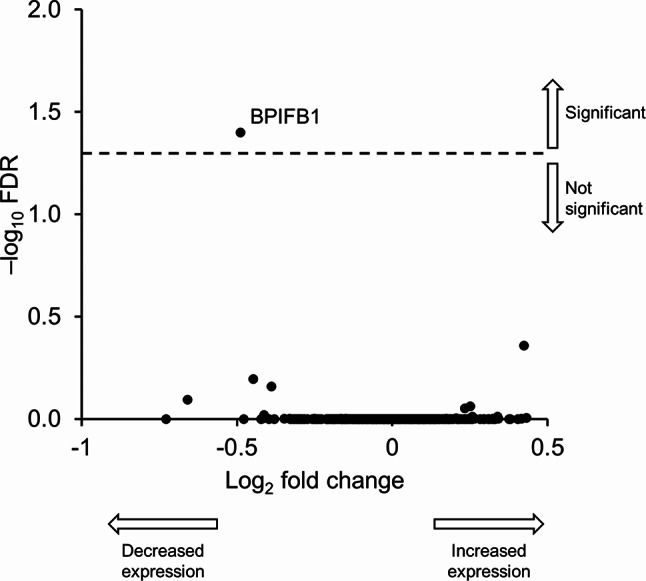
Results: CHF6523 plasma pharmacokinetics were characterised by an early maximum concentration (Cmax), reached 15 and 10 min after dosing on Days 1 and 28, respectively, followed by a rapid decline. Systemic exposure on Day 28 showed limited accumulation, with ratios < 1.6 for Cmax and area under the curve from 0 to 12 h post-dose, and with steady state achieved on Day 20. Target engagement was confirmed by a significant 29.7% reduction from baseline in induced sputum PIP3 (29.5% reduction vs. placebo; adjusted ratio 0.705 [0.580, 0.856]; p = 0.001), but this did not translate into an anti-inflammatory pharmacodynamic effect, as assessed through measures including biomarkers and multi-omics. Additionally, although CHF6523 was generally well-tolerated, 95.2% of patients reported cough as an adverse event, most mild to moderate and resolving within one-hour post-dose.
Conclusions: These data, together with those from other PI3K inhibitors, suggest that PI3Kδ is not a suitable pathway for the management of COPD, as the achieved target engagement did not translate into any pharmacodynamic anti-inflammatory effect.
Trial registration: ClinicalTrials.gov (NCT04032535); posted 23rd July 2019.
Keywords: Gene expression profiling; Multi-omics; Phosphatidylinositol 3-kinases; Proteomics; Therapeutics.
© 2024. The Author(s).
Conflict of interest statement
MG, MBa, GL, FR, RC, DG, MLF, BP, RB, and DM are employees of Chiesi, the sponsor of this study, LG was engaged as a consultant by Chiesi, and GM and MBo were employees of Chiesi at the time the study was conducted. JC declares a contract and payment to the Babraham Institute for analysis of sputum PIP3 by mass spectrometry. Outside the scope of the manuscript, he has no conflicts to disclose. FP has no other conflicts to disclose. AMK declares that her employer was contracted for the clinical work in this study. She has no other conflicts to disclose. KMB declares consulting fees from Berlin Chemie, Sanofi, Bosch Healthcare, and Clario, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Berlin Chemie, GlaxoSmithKline, AstraZeneca, Sanofi, and Orion, and participation on a data safety monitoring board or advisory board for Chiesi and GlaxoSmithKline, all outside the scope of the current manuscript. OK declares payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from AstraZeneca and Novartis, and participation on a data safety monitoring board or advisory board for Sanofi, all outside the scope of the current manuscript. SK declares consulting fees, participation in advisory boards, and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, and Sanofi, all outside the scope of the current manuscript. ALS has no other conflicts to disclose. HW declares that his employer was contracted for the clinical work in this study. Outside the scope of the current manuscript he declares consulting fees, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events, support for attending meetings and/or travel, and participation on a data safety monitoring board or advisory board, all for AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, and Sanofi. In addition, he is a speaker in COPD for the German Center for Lung Research.
Figures


References
-
- Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease [Internet]. 2024 [cited 2024 Jun 10]. https://goldcopd.org/2024-gold-report/
-
- Adcock IM, Caramori G. Kinase targets and inhibitors for the treatment of airway inflammatory diseases: the next generation of drugs for severe asthma and COPD? BioDrugs 2004;18:167–80. 10.2165/00063030-200418030-00003/METRICS - PubMed
-
- Ito K, Caramori G, Adcock IM. Therapeutic potential of phosphatidylinositol 3-kinase inhibitors in inflammatory respiratory disease. J Pharmacol Exp Ther. 2007;321:1–8. 10.1124/JPET.106.111674. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
