

Role of cuproptosis in mediating the severity of experimental malaria-associated acute lung injury/acute respiratory distress syndrome
- PMID: 39427197
- PMCID: PMC11489997
- DOI: 10.1186/s13071-024-06520-1
Role of cuproptosis in mediating the severity of experimental malaria-associated acute lung injury/acute respiratory distress syndrome
Abstract
Background: Malaria-associated acute lung injury/acute respiratory distress syndrome (MA-ALI/ARDS) is a fatal complication of Plasmodium falciparum infection that is partially triggered by macrophage recruitment and polarization. As reported, copper exposure increases the risk of malaria infection, and copper accumulation-induced cuproptosis triggers M1 macrophage polarization. It is thus hypothesized that cuproptosis could act as a critical mediator in the pathogenesis of MA-ALI/ARDS, but its underlying mechanism remains unclear. The present study aimed to explore the role of cuproptosis in the severity of murine MA-ALI/ARDS.
Methods: We utilized an experimental model of MA-ALI/ARDS using female C57BL/6 mice with P. berghei ANKA infection, and treated these animals with the potent copper ion carrier disulfiram (DSF) or copper ion chelator tetrathiomolybdate (TTM). The RAW 264.7 macrophages, which were stimulated with infected red blood cells (iRBCs) in vitro, were also targeted with DSF-CuCl2 or TTM-CuCl2 to further investigate the underlying mechanism.
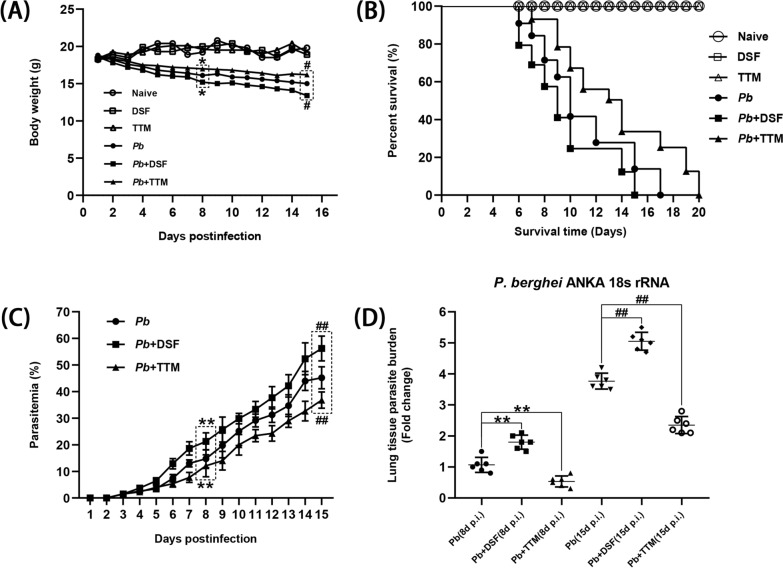
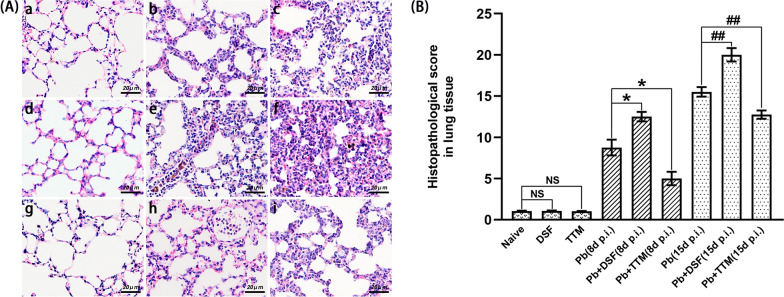
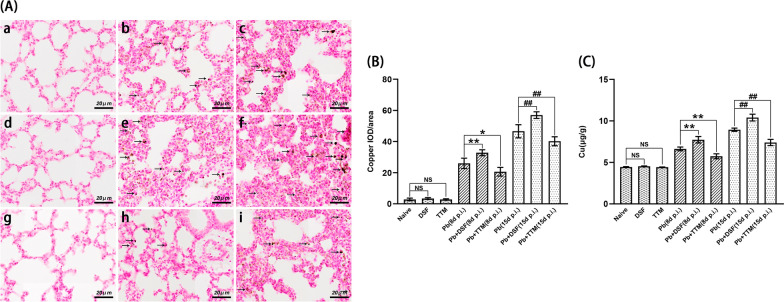
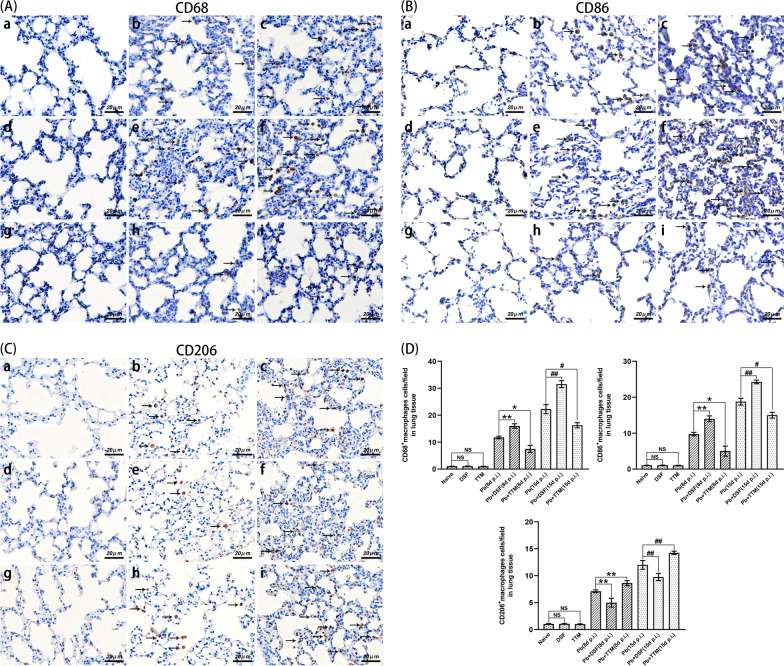
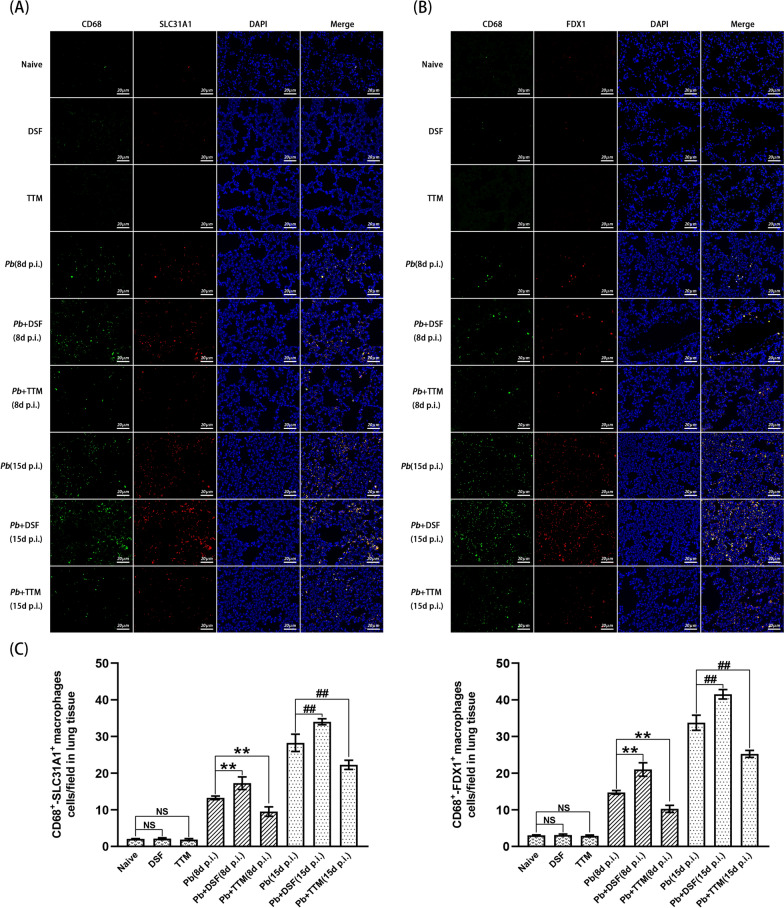
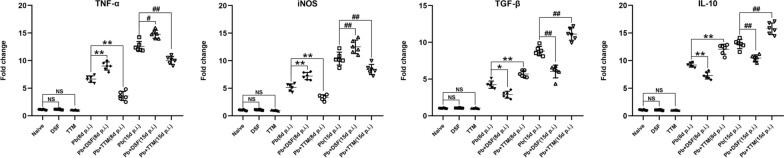
Results: Our findings showed a dramatic elevation in the amount of copper and the expression of SLC31A1 (a copper influx transporter) and FDX1 (a key positive regulator of cuproptosis) but displayed a notable reduction in the expression of ATP7A (a copper efflux transporter) in the lung tissue of experimental MA-ALI/ARDS mice. Compared to the P. berghei ANKA-infected control group, mice that were administered DSF exhibited a remarkable increase in parasitemia/lung parasite burden, total protein concentrations in bronchoalveolar lavage fluid (BALF), lung wet/dry weight ratio, vascular leakage, and pathological changes in lung tissue. Strikingly, the experimental MA-ALI/ARDS mice with DSF treatment also demonstrated dramatically elevated copper levels, expression of SLC31A1 and FDX1, numbers of CD86+, CD68+, SLC31A1+-CD68+, and FDX1+-CD68+ macrophages, and messenger RNA (mRNA) levels of pro-inflammatory cytokines (tumor necrosis factor [TNF-α] and inducible nitric oxide synthase [iNOS]) in lung tissue, but showed a remarkable decrease in body weight, survival time, expression of ATP7A, number of CD206+ macrophages, and mRNA levels of anti-inflammatory cytokines (transforming growth factor beta [TGF-β] and interleukin 10 [IL-10]). In contrast, TTM treatment reversed these changes in the infected mice. Similarly, the in vitro experiment showed a notable elevation in the mRNA levels of SLC31A1, FDX1, CD86, TNF-α, and iNOS in iRBC-stimulated RAW 264.7 cells targeted with DSF-CuCl2, but triggered a remarkable decline in the mRNA levels of ATP7A, CD206, TGF-β, and IL-10. In contrast, TTM-CuCl2 treatment also reversed these trends in the iRBC-stimulated RAW 264.7 cells.
Conclusions: Our data demonstrate that the activation of cuproptosis with DSF aggravated the severity of MA-ALI/ARDS by partially inducing M1 polarization of pulmonary macrophages, while inhibition of cuproptosis with TTM contrarily ameliorated the severity of MA-ALI/ARDS by promoting macrophage M2 polarization. Our findings suggest that blockage of cuproptosis could be a potential therapeutic strategy for treatment of MA-ALI/ARDS.
Keywords: ALI/ARDS; Cuproptosis; M1/M2 polarization; Macrophage; Malaria.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- WHO. World Malaria Report 2023. Geneva: World Health Organization. 2023.
-
- Balaji SN, Deshmukh R, Trivedi V. Severe malaria: biology, clinical manifestation, pathogenesis and consequences. J Vector Borne Dis. 2020;57:1–13. - PubMed
-
- Siagian FE. Pulmonary complication in severe malaria. IJPR. 2021;8:19–27.
-
- Taylor WRJ, Hanson J, Turner GDH, White NJ, Dondorp AM. Respiratory manifestations of malaria. Chest. 2012;142:492–505. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
