

Inference-Based Cognitive Behavioral Therapy versus Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder: A Multisite Randomized Controlled Non-Inferiority Trial
- PMID: 39427635
- PMCID: PMC11614422
- DOI: 10.1159/000541508
Inference-Based Cognitive Behavioral Therapy versus Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder: A Multisite Randomized Controlled Non-Inferiority Trial
Abstract
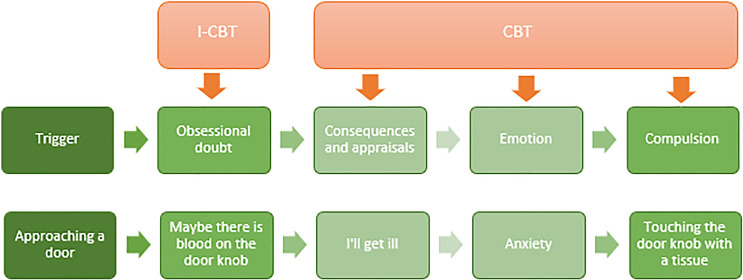
Introduction: Although cognitive behavioral therapy (CBT) effectively treats obsessive-compulsive disorder (OCD), many patients refuse CBT or drop out prematurely, partly because of anxiety regarding exposure and response prevention (ERP) exercises. Inference-based cognitive behavioral therapy (I-CBT) focuses on correcting distorted inferential thinking patterns, enhancing reality-based reasoning, and addressing obsessional doubt by targeting underlying dysfunctional reasoning, without incorporating an ERP component. We hypothesized that I-CBT would be non-inferior to CBT. Additionally, we hypothesized that I-CBT would be more tolerable than CBT.
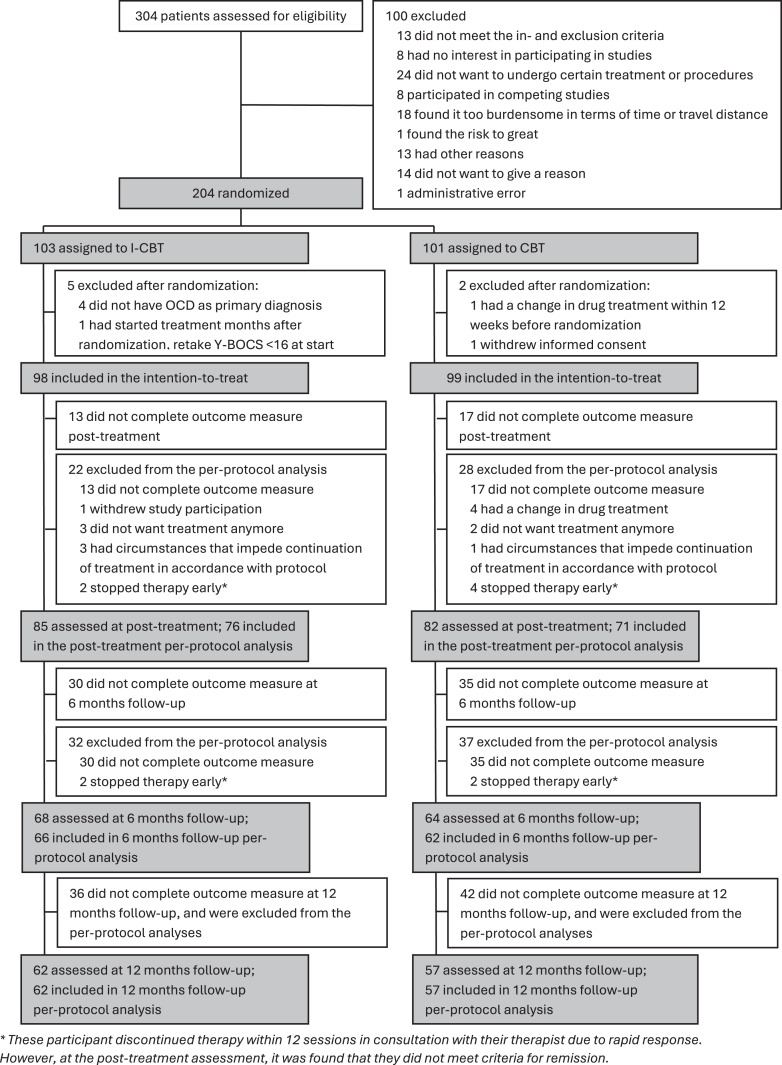
Methods: 197 participants were randomly assigned to 20 sessions CBT or I-CBT and assessed at baseline, posttreatment, and 6 and 12 months' follow-up. The primary outcome was OCD symptom severity measured using the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS; non-inferiority margin: 2 points). The secondary outcome, treatment tolerability, was assessed using the Treatment Acceptability/Adherence Scale (TAAS). A linear mixed-effects model was used to assess the non-inferiority of the primary outcome and superiority of secondary outcomes.
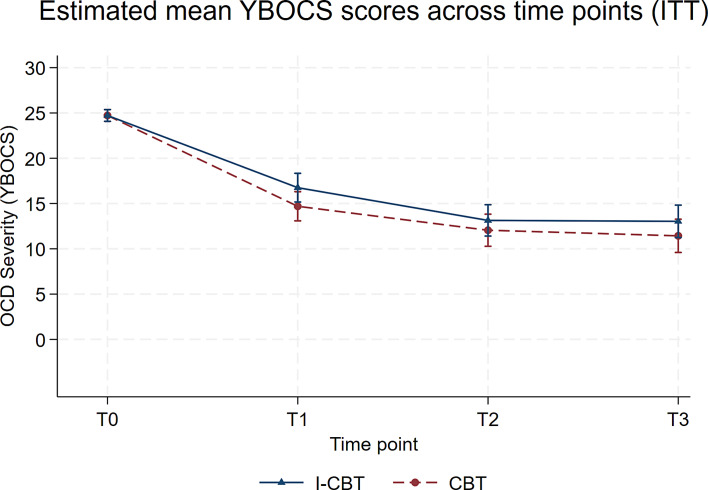
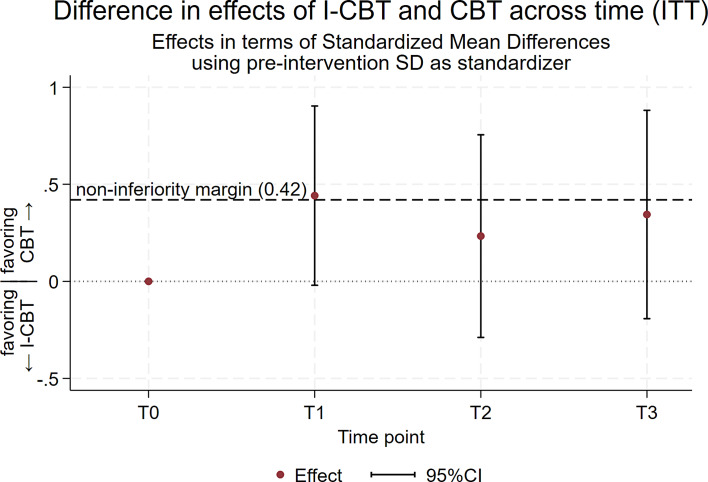
Results: Statistically significant within-group improvements in the primary and secondary outcomes were observed in both treatments. No statistically significant between-group differences in Y-BOCS were found at any assessment point, but the confidence intervals exceeded the non-inferiority threshold, making the results inconclusive. The estimated mean posttreatment TAAS score was significantly higher in the I-CBT group than in the CBT group.
Conclusion: While both CBT and I-CBT are effective for OCD, whether I-CBT is non-inferior to CBT in terms of OCD symptom severity remains inconclusive. Nevertheless, I-CBT offers better tolerability and warrants consideration as an alternative treatment for OCD.
Keywords: Cognitive behavioral therapy; Inference-based cognitive behavioral therapy; Obsessive-compulsive disorder; Psychiatric disorders; Treatment outcome.
© 2024 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Visser HA, van Oppen P, van Megen HJ, Eikelenboom M, van Balkom AJ. Obsessive-compulsive disorder; chronic versus non-chronic symptoms. J Affect Disord. 2014;152–154(1):169–74. - PubMed
-
- Cicek E, Cicek IE, Kayhan F, Uguz F, Kaya N. Quality of life, family burden and associated factors in relatives with obsessive–compulsive disorder. Gen Hosp Psychiatry. 2013;35(3):253–8. - PubMed
-
- Remmerswaal KCP, Batelaan NM, Smit JH, van Oppen P, van Balkom AJLM. Quality of life and relationship satisfaction of patients with Obsessive Compulsive Disorder. J Obsessive Compuls Relat Disord. 2016;11:56–62.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
