

Perinatal Caffeine Administration Improves Outcomes in an Ovine Model of Neonatal Hypoxia-Ischemia
- PMID: 39429154
- PMCID: PMC11518658
- DOI: 10.1161/STROKEAHA.124.048264
Perinatal Caffeine Administration Improves Outcomes in an Ovine Model of Neonatal Hypoxia-Ischemia
Abstract
Background: Neonatal hypoxic-ischemic encephalopathy disproportionately affects low- and middle-income countries, where ≈96% of affected infants reside. The current standard of care, therapeutic hypothermia, is frequently ineffective in this setting, likely because injury may be occurring earlier during labor. Here, we studied the pharmacokinetics, safety, and efficacy of perinatal caffeine administration in near-term lambs following global ischemic injury to support the development of earlier treatment strategies targeting the fetus in utero as well as the infant postnatally.
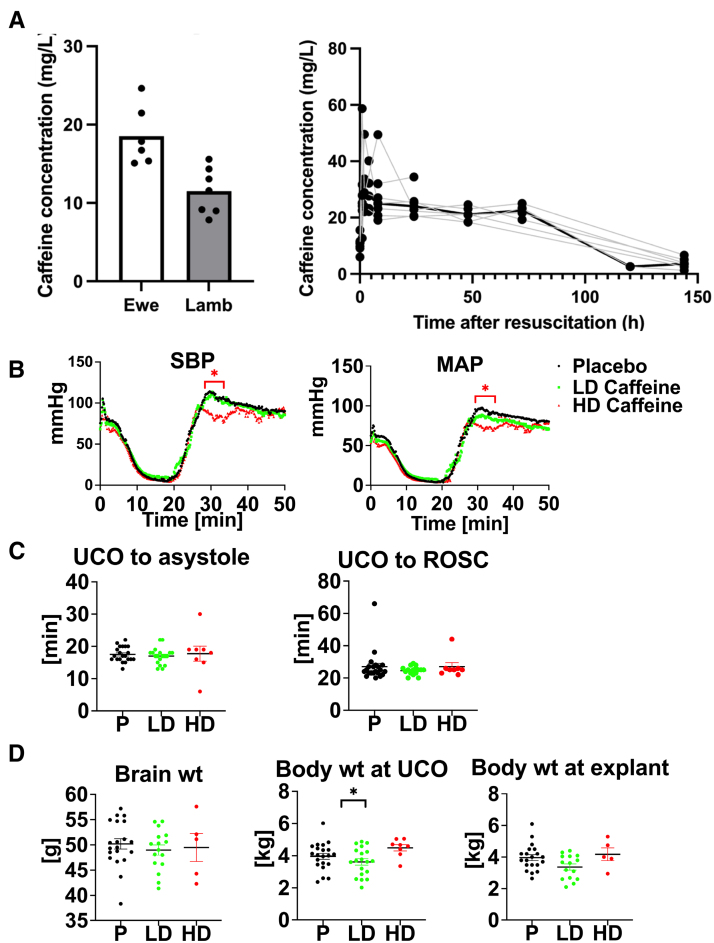
Methods: Ewes were randomly assigned to receive either 1 g IV caffeine citrate or placebo before delivery and placental transport assessed. Near-term lambs (141-143 days) of both sexes were subjected to severe global hypoxia-ischemia utilizing an acute umbilical cord occlusion model. Lambs that received caffeine in utero also received 20 mg/kg IV caffeine citrate following resuscitation and 10 mg/(kg·d) IV for 2 days. An additional cohort received 60 mg/kg followed by 30 mg/(kg·d) (low dose versus high dose) postnatally. Biochemical, histological, and neurological outcome measures in lambs were assessed over a 6-day period.
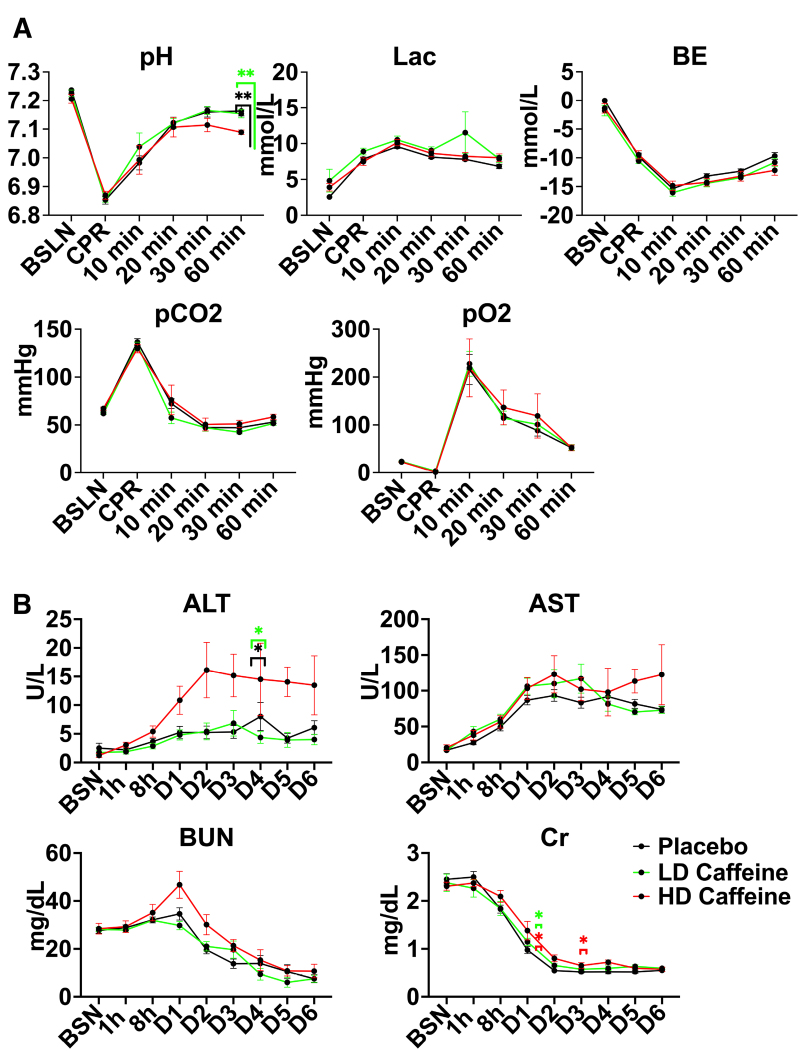
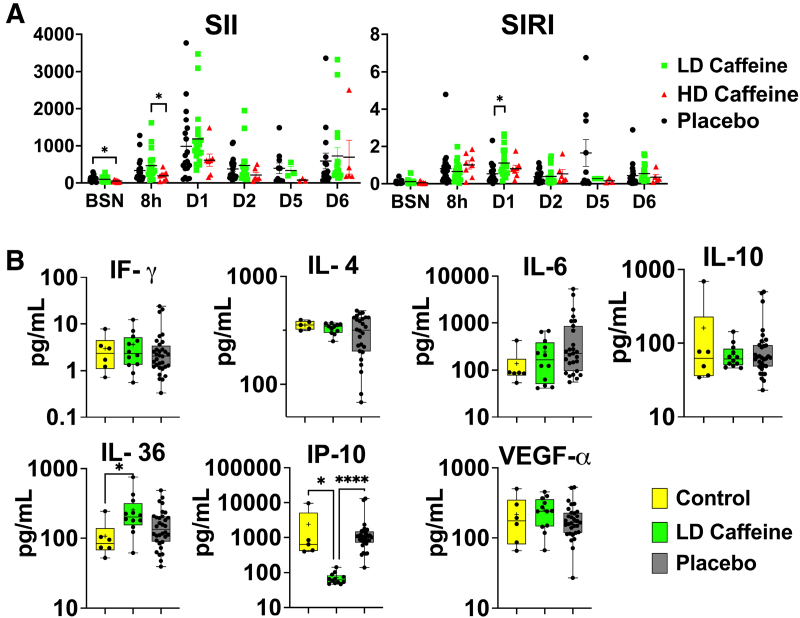
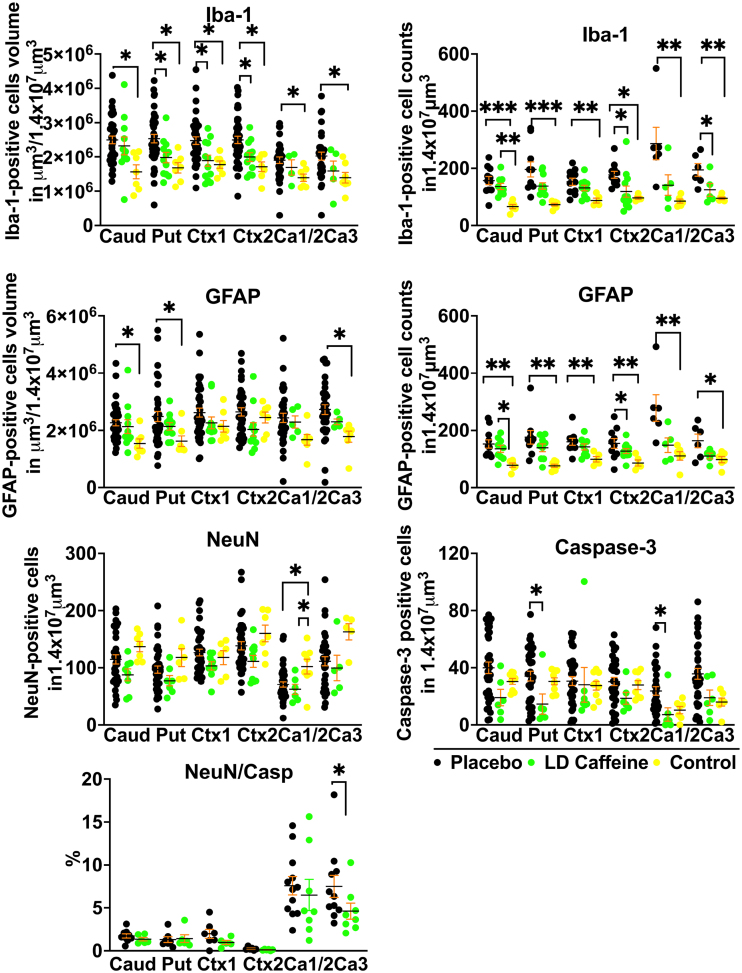
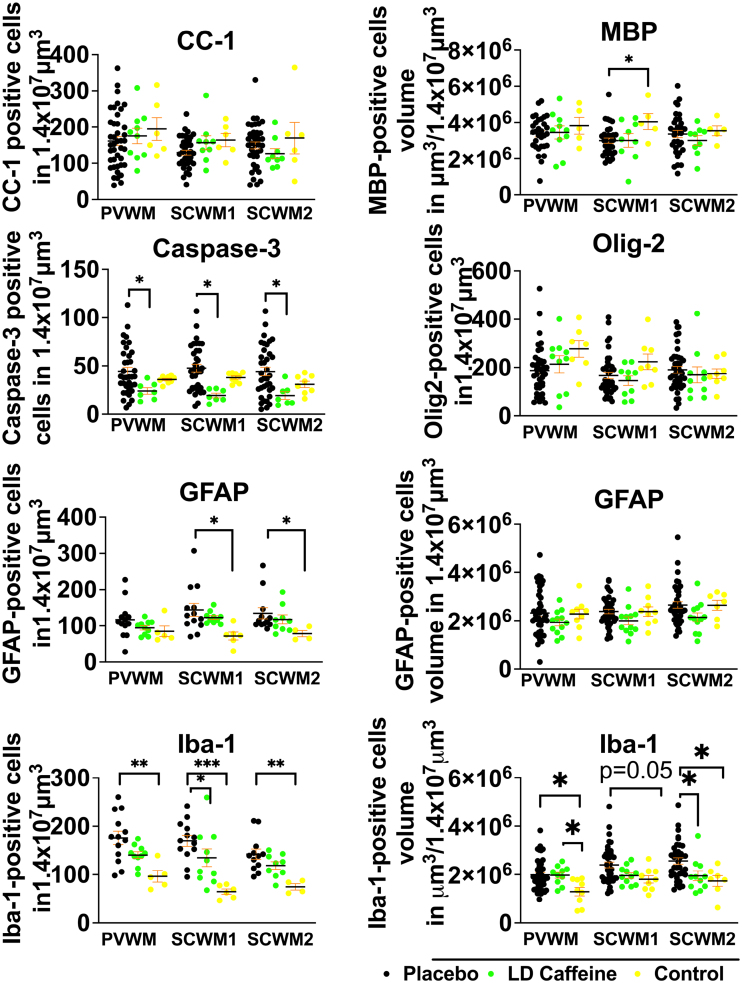
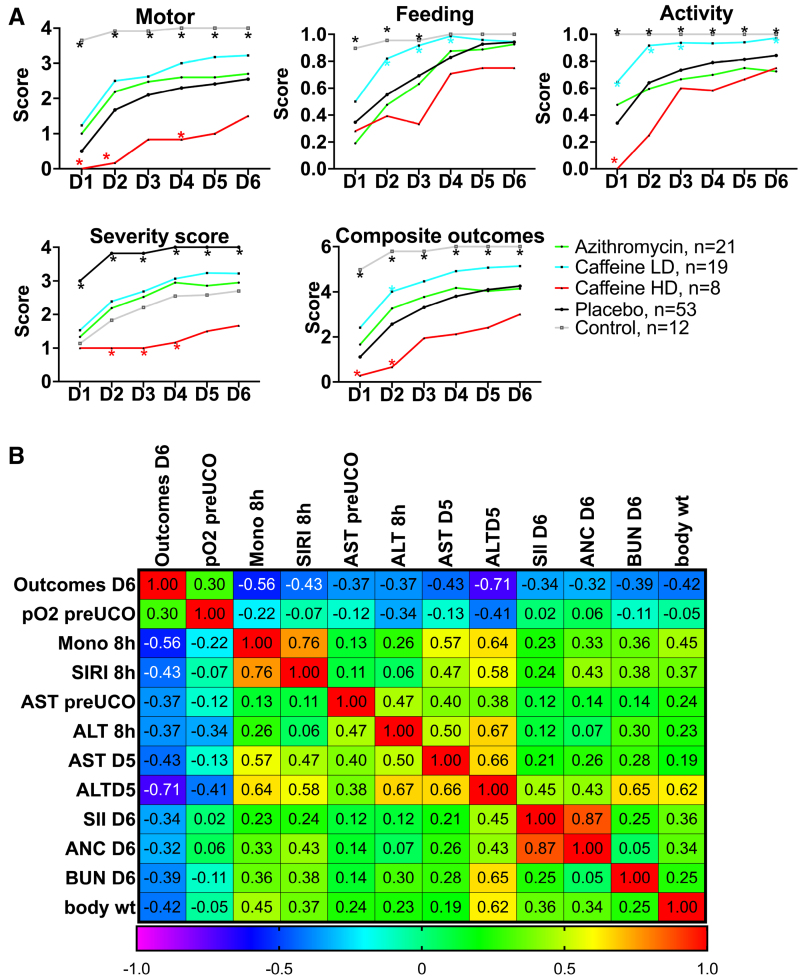
Results: Perinatal caffeine administration demonstrated excellent placental transport kinetics and was well tolerated with lamb plasma levels comparable to those targeted in neonates with apnea of prematurity. Caffeine administration resulted in a systemic immunomodulatory effect, evidenced by significant reductions in proinflammatory IP-10 levels. Treated lambs demonstrated improved neurodevelopmental outcomes, while histological analysis revealed that caffeine reduced gray matter injury and attenuated inflammation in the cingulate and parasagittal cortex. This neuroprotective effect was greater and via a different mode of action than we previously reported for azithromycin. A higher caffeine dosing regimen demonstrated significant toxicity.
Conclusions: Perinatal caffeine administration is well tolerated, attenuates systemic and brain inflammation, and contributes to improvements in histological and neurological outcomes in an ovine model of neonatal hypoxic-ischemic encephalopathy.
Keywords: caffeine; developing countries; gray matter; hypoxia-ischemia, brain; sheep.
Conflict of interest statement
None.
Figures
References
-
- Thayyil S, Pant S, Montaldo P, Shukla D, Oliveira V, Ivain P, Bassett P, Swamy R, Mendoza J, Moreno-Morales M, et al. ; HELIX Consortium. Hypothermia for moderate or severe neonatal encephalopathy in low-income and middle-income countries (HELIX): a randomised controlled trial in India, Sri Lanka, and Bangladesh. Lancet Glob Health. 2021;9:e1273–e1285. doi: 10.1016/S2214-109X(21)00264-3 - PMC - PubMed
