

EUS-guided hepaticogastrostomy: practical tips and tricks
- PMID: 39429912
- PMCID: PMC11489514
- DOI: 10.1016/j.vgie.2024.05.015
EUS-guided hepaticogastrostomy: practical tips and tricks
Abstract
Background and aims: EUS-guided hepaticogastrostomy (EUS-HGS) has gained traction as a reliable and safe method for definitive biliary drainage in patients who cannot undergo traditional transampullary procedures. Many of the newly developed single-stage devices are not yet approved for clinical use in Western practice.
Methods: We highlight key clinical and technical aspects of EUS-HGS using devices that are currently available in Western countries. The article is a comprehensive step-by-step technical review of EUS-HGS, and the video demonstrates high-level tips to overcome commonly encountered procedural challenges.
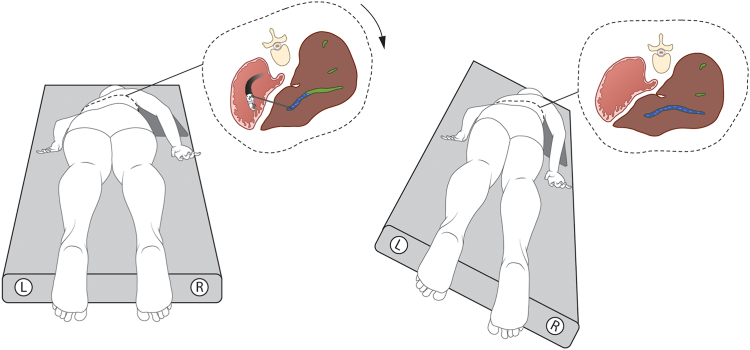
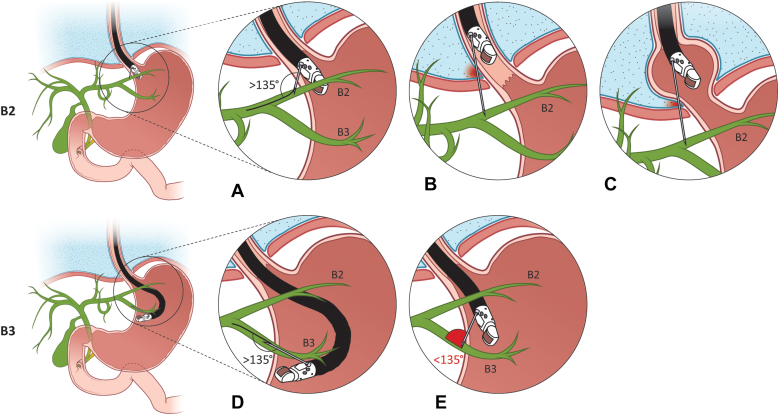
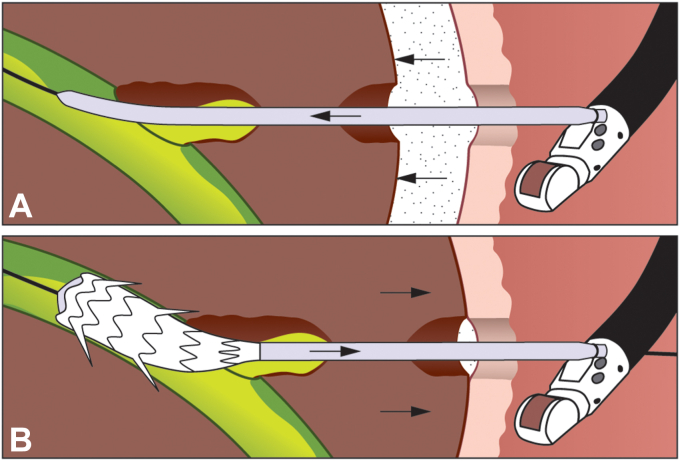
Results: Patients with biliary obstruction underwent EUS-HGS at our center. The technical difficulties that were encountered are highlighted in the article and the accompanying video. The article and video provide a detailed review of (1) preprocedural considerations, (2) puncture site selection, (3) biliary puncture, (4) contrast injection, (5) guidewire manipulation, (6) tract dilation, and (7) stent placement.
Conclusion: An understanding and implementation of the technical nuances highlighted in this article should help Western endoscopists navigate the complexities of EUS-HGS and ensure optimal outcomes.
© 2024 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc.
Conflict of interest statement
Dr Irani is a consultant for Boston Scientific, WL Gore & Associates. The other author disclosed no financial relationships relevant to this publication.
Figures







References
-
- Burmester E., Niehaus J., Leineweber T., Huetteroth T. EUS-cholangio-drainage of the bile duct: report of 4 cases. Gastrointest Endosc. 2003;57:246–251. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
