

Giant Chondromyxoid Fibroma Associated With Epileptic Seizures: A Case Report
- PMID: 39429986
- PMCID: PMC11488528
- DOI: 10.7759/cureus.70950
Giant Chondromyxoid Fibroma Associated With Epileptic Seizures: A Case Report
Abstract
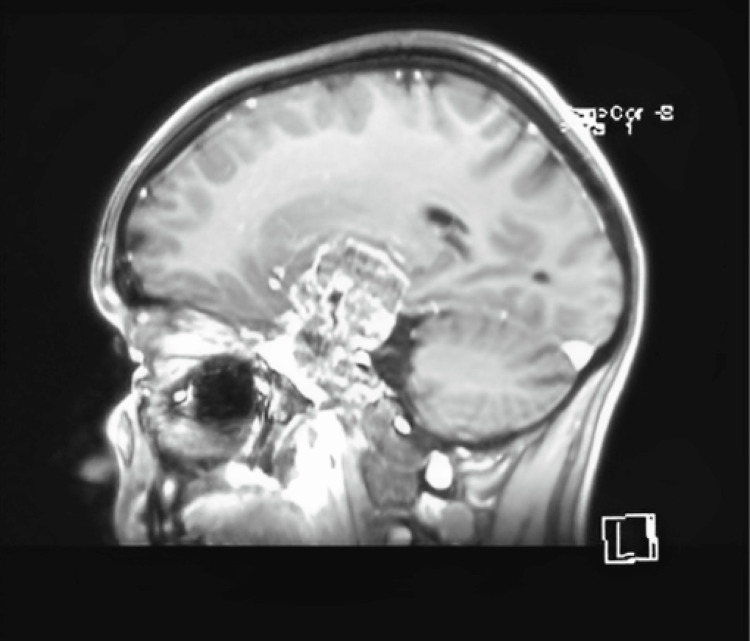
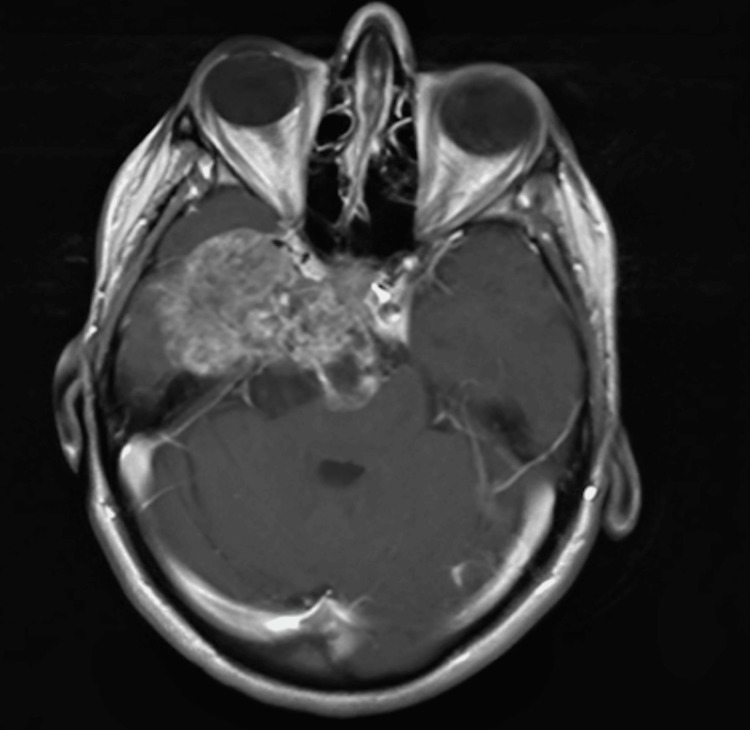
This case report presents an exceedingly rare instance of skull base chondromyxoid fibroma (CMF) managed surgically. Chondromyxoid fibromas are very rare tumors (<1% of benign bone tumors), the occurrence in the skull area being even more rare. The location of tumors at the skull base makes their surgical resection extremely challenging, usually resulting in subtotal resection (STR). One aspect that makes this case stand out is its unique clinical presentation, particularly the presence of epileptic seizures. Patients suffering from skull base CMFs must receive regular follow-up exams in order to track disease progress, maintain quality of life, and prevent further complications.
Keywords: chondromyxoid fibroma; epileptic seizures; neurosurgery; skull base; subtotal resection.
Copyright © 2024, Toader et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Chondromyxoid Fibroma of the Skull Base and Calvarium: Surgical Management and Literature Review.J Neurol Surg Rep. 2016 Mar;77(1):e023-34. doi: 10.1055/s-0035-1570033. Epub 2016 Jan 4. J Neurol Surg Rep. 2016. PMID: 26929898 Free PMC article.
-
Chondromyxoid fibroma of zygomatic bone: A case report.Ann Med Surg (Lond). 2022 Feb 22;75:103394. doi: 10.1016/j.amsu.2022.103394. eCollection 2022 Mar. Ann Med Surg (Lond). 2022. PMID: 35251603 Free PMC article.
-
Chondromyxoid fibroma of the mandible: Case report and review of the literature.Ann Maxillofac Surg. 2014 Jan;4(1):78-80. doi: 10.4103/2231-0746.133072. Ann Maxillofac Surg. 2014. PMID: 24987604 Free PMC article.
-
Chondromyxoid fibroma of the skull base: differential diagnosis and radiotherapy: two case reports and a review of the literature.Acta Oncol. 2005;44(6):545-53. doi: 10.1080/00365590500237846. Acta Oncol. 2005. PMID: 16165913 Review.
-
Chondromyxoid fibroma-like osteosarcoma: a case series and literature review.BMC Musculoskelet Disord. 2020 Jan 29;21(1):53. doi: 10.1186/s12891-020-3063-5. BMC Musculoskelet Disord. 2020. PMID: 31996205 Free PMC article. Review.
Cited by
-
Precision Neuro-Oncology in Glioblastoma: AI-Guided CRISPR Editing and Real-Time Multi-Omics for Genomic Brain Surgery.Int J Mol Sci. 2025 Jul 30;26(15):7364. doi: 10.3390/ijms26157364. Int J Mol Sci. 2025. PMID: 40806492 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources