

Lower Parathyroid Hormone Levels are Associated With Reduced Fracture Risk in Japanese Patients on Hemodialysis
- PMID: 39430172
- PMCID: PMC11489479
- DOI: 10.1016/j.ekir.2024.07.008
Lower Parathyroid Hormone Levels are Associated With Reduced Fracture Risk in Japanese Patients on Hemodialysis
Erratum in
-
Corrigendum to "Lower Parathyroid Hormone Levels are Associated With Reduced Fracture Risk in Japanese Patients on Hemodialysis" [Kidney International Reports Volume 9, Issue 10, October 2024, Pages 2956-2969].Kidney Int Rep. 2025 May 14;10(7):2495. doi: 10.1016/j.ekir.2025.05.010. eCollection 2025 Jul. Kidney Int Rep. 2025. PMID: 40677350 Free PMC article.
Abstract
Introduction: Secondary hyperparathyroidism (SHPT) affects bone metabolism and may lead to bone fragility. However, there is conflicting evidence as to whether parathyroid hormone (PTH) levels are associated with fracture risk and whether the relationship is linear or U-shaped.
Methods: We examined the association between PTH levels and the risk of any fracture and site-specific fractures in a nationwide cohort of 180,333 patients on hemodialysis. We also examined the association between the percent change in PTH levels during the preceding 1 year and subsequent fracture.
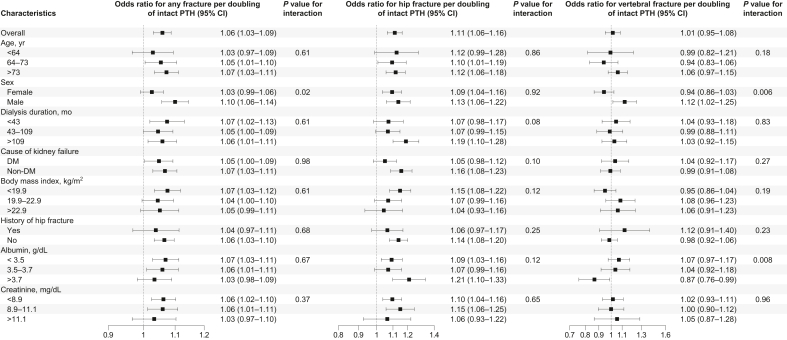
Results: At baseline, the median intact PTH level was 141 pg/ml (interquartile range, 78-226 pg/ml). During 1 year of follow-up, there were a total of 3762 fractures requiring hospitalization (1361 hip, 551 vertebral, and 1850 other). In an adjusted analysis, higher baseline PTH levels were associated with an incrementally increased risk of any fracture (odds ratio [OR] per doubling of intact PTH, 1.06; 95% confidence interval, 1.03-1.09). The association between PTH levels and fracture risk was more pronounced for hip fractures but not found for vertebral fractures. The absolute risk difference associated with higher PTH levels appeared to be more pronounced in older individuals, females, and those with lower body mass index (BMI). Change in PTH levels was also associated with fracture risk: the adjusted OR for fracture decreased linearly with decreasing PTH levels over 1 year, regardless of the preceding PTH levels.
Conclusion: Lower PTH levels are associated with a graded reduction in fracture risk. Further studies are needed to determine whether intensive PTH control reduces fracture risk.
Keywords: fracture; hemodialysis; parathyroid hormone; secondary hyperparathyroidism.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures






References
-
- Yamamoto S., Karaboyas A., Komaba H., et al. Mineral and bone disorder management in hemodialysis patients: comparing PTH control practices in Japan with Europe and North America: the Dialysis Outcomes and Practice Patterns Study (DOPPS) BMC Nephrol. 2018;19:253. doi: 10.1186/s12882-018-1056-5. - DOI - PMC - PubMed
-
- Kidney disease: improving global outcomes (KDIGO) CKD-MBD update work group KDIGO 2017 clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD) Kidney Int Suppl (2011) 2017;(7):1–59. doi: 10.1016/j.kisu.2017.04.001. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
