

Paradoxical restoration from complete and persistent atrioventricular block after surgical aortic valve replacement: a case report
- PMID: 39430673
- PMCID: PMC11489870
- DOI: 10.1093/ehjcr/ytae549
Paradoxical restoration from complete and persistent atrioventricular block after surgical aortic valve replacement: a case report
Abstract
Background: One of the most important and relatively frequent complications of aortic valve replacement is atrioventricular block. It typically occurs by direct injury of the infranodal conduction system due to intra-operative manipulation and persists post-operatively, necessitating permanent pacemaker implantation in many cases.
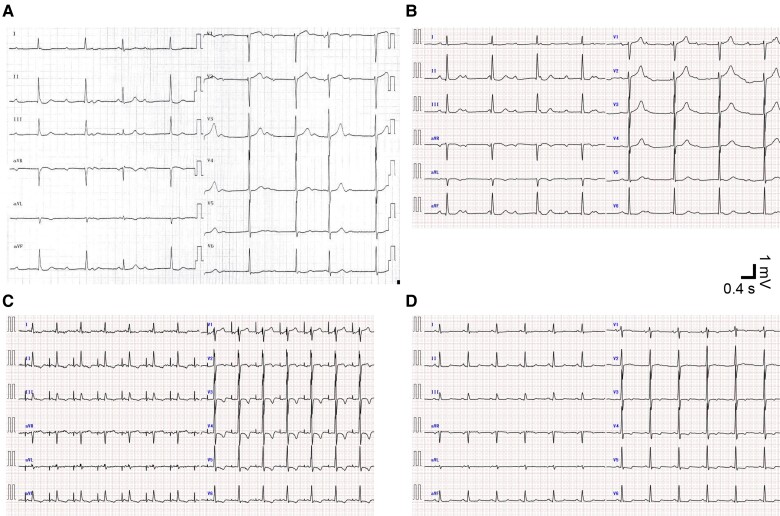
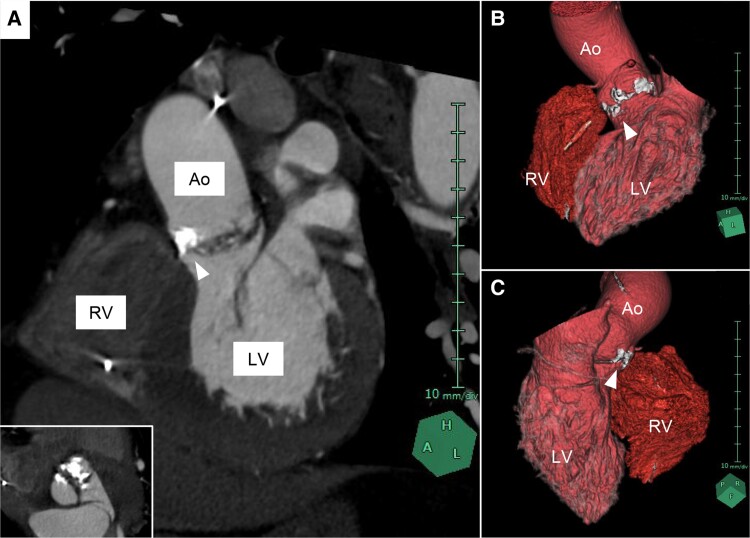
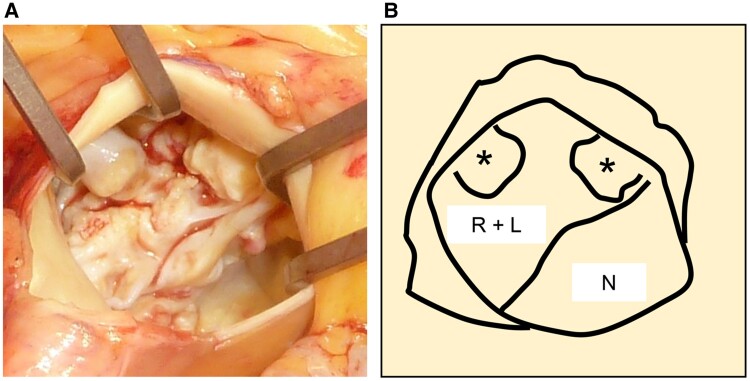
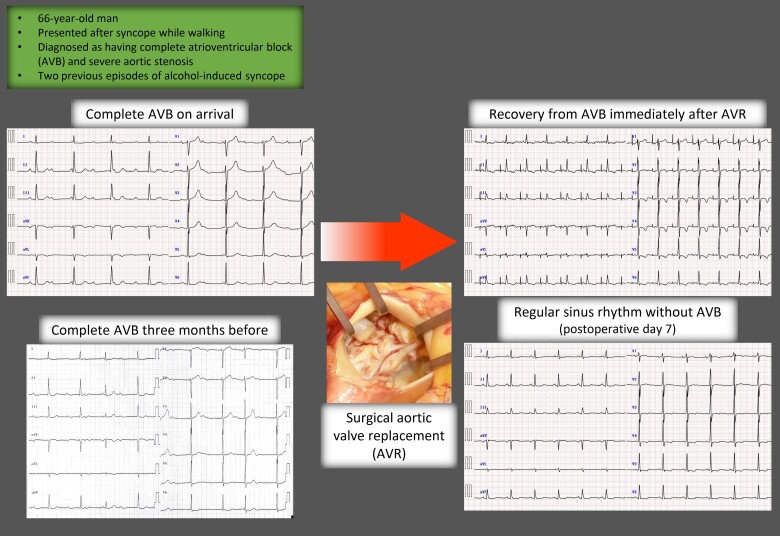
Case summary: A 66-year-old man presented to our hospital after experiencing syncope while walking after drinking. He had experienced two episodes of alcohol-induced syncope several years earlier. His electrocardiogram (ECG) and transthoracic echocardiogram revealed complete atrioventricular block and severe aortic stenosis, respectively. He received a temporary pacemaker on the day of admission and underwent surgical aortic valve replacement on hospital Day 9. The native aortic valve was bicuspid. Unexpectedly, the ECG immediately after aortic valve replacement showed complete restoration of atrioventricular conduction during temporary atrial pacing. The atrioventricular block did not recur, and he was discharged to home on post-operative Day 13.
Discussion: This remarkably rare clinical course, complete restoration from complete and persistent atrioventricular block after surgical aortic valve replacement, can be explained by multifactorial mechanisms: (i) surgical removal of the aortic annulus calcification directly hindering the infranodal conduction system; (ii) relief from the ventricular pressure overload stressing the conduction system within the septum; and (iii) improvement of substantial autonomic dysregulation as manifested by alcohol-sensitive syncope in the present patient, which was a result of unloading of the intraventricular pressure affecting the left ventricular mechanoreceptor.
Keywords: Aortic stenosis; Aortic valve replacement; Case report; Complete atrioventricular block; Syncope.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest:. None declared.
Figures
References
-
- Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, et al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J 2021;42:3427–3520. - PubMed
-
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2022;43:561–632. - PubMed
-
- Misumida N, Pagath M, Ogunbayo GO, Wilson RE, Kim SM, Abdel-Latif A, et al. Characteristics of and current practice patterns of pacing for high-degree atrioventricular block after transcatheter aortic valve implantation in comparison to surgical aortic valve replacement. Catheter Cardiovasc Interv 2019;93:E385–E390. - PMC - PubMed
-
- Pakrashi BC, Mary DA, Garcia JB, Ionescu MI. Recovery from complete heart block following aortic valve replacement. Arch Surg 1974;108:373–375. - PubMed
-
- Francisco-Pascual J, Rodenas E, Belahnech Y, Rivas-Gándara N, Pérez-Rodon J, Santos-Ortega A, et al. Syncope in patients with severe aortic stenosis: more than just an obstruction issue. Can J Cardiol 2021;37:284–291. - PubMed
Publication types
LinkOut - more resources
Full Text Sources