

Hyperfibrinolysis: a crucial phenotypic abnormality of posttraumatic fibrinolytic dysfunction
- PMID: 39430866
- PMCID: PMC11488401
- DOI: 10.1016/j.rpth.2024.102568
Hyperfibrinolysis: a crucial phenotypic abnormality of posttraumatic fibrinolytic dysfunction
Abstract
Background: Traumatic fibrinolytic dysfunction is often categorized into 3 phenotypes based on the result of thromboelastography (TEG) lysis at 30 minutes (LY30): fibrinolysis shutdown, physiologic fibrinolysis, and hyperfibrinolysis. However, the molecular pathophysiology of fibrinolytic dysfunction and the association with clinical outcomes have not been fully evaluated.
Objectives: To assess whether posttraumatic fibrinolysis phenotypes identified by TEG correlate with levels of key fibrinolysis-related serum markers and with risk of mortality and hospital complications.
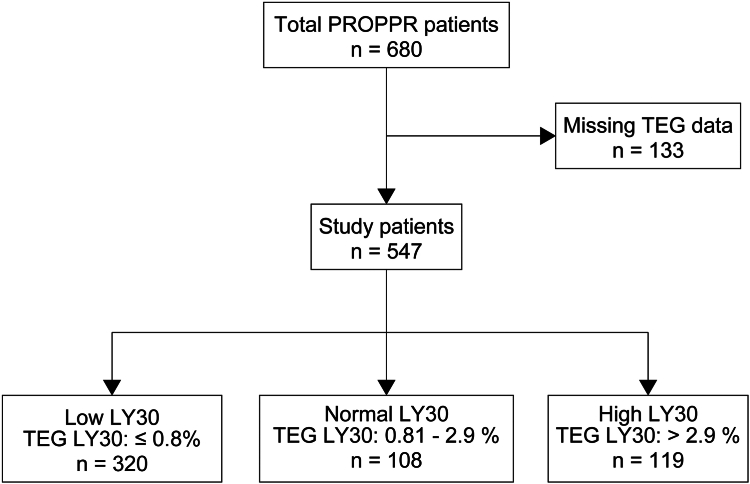
Methods: This is a secondary analysis of the Pragmatic, Randomized Optimal Platelet and Plasma Ratios trial. Patients were stratified according to the degree of fibrinolysis upon arrival using TEG LY30 values: low LY30, <0.8%; normal LY30, 0.81% to 0.9%; and high LY30, ≥3%. Serial values of molecular markers (0-72 hours after admission) and clinical outcomes were compared between fibrinolysis groups.
Results: A total of 547 patients were included (low LY30, 320; normal LY30, 108; high LY30, 119). The high LY30 group had higher tissue plasminogen activator and plasmin-antiplasmin values upon hospital arrival than the low LY30 or normal LY30 groups (P < .001, respectively). There was no significant difference in levels of tissue plasminogen activator, plasmin-antiplasmin, and plasminogen activator inhibitor 1 between the low LY30 and normal LY30 groups. The high LY30 group was associated with an increased risk of 24-hour and 30-day mortality, while there was no significant difference in mortality between the low LY30 and normal LY30 groups.
Conclusion: Our results suggest that hyperfibrinolysis is the most common form of traumatic fibrinolytic dysfunction and is associated with worse outcome.
Keywords: blood transfusion; hyperfibrinolysis; outcome; thromboelastography; trauma-induced coagulopathy.
© 2024 The Authors.
Figures


References
-
- Sauaia A., Moore F.A., Moore E.E., Moser K.S., Brennan R., Read R.A., et al. Epidemiology of trauma deaths: a reassessment. J Trauma. 1995;38:185–193. - PubMed
-
- Hayakawa M., Gando S., Ono Y., Wada T., Yanagida Y., Sawamura A. Fibrinogen level deteriorates before other routine coagulation parameters and massive transfusion in the early phase of severe trauma: a retrospective observational study. Semin Thromb Hemost. 2015;41:35–42. - PubMed
-
- Kashuk J.L., Moore E.E., Sawyer M., Wohlauer M., Pezold M., Barnett C., et al. Primary fibrinolysis is integral in the pathogenesis of the acute coagulopathy of trauma. Ann Surg. 2010;252:434–442. discussion 443. - PubMed
-
- Moore H.B., Moore E.E., Gonzalez E., Chapman M.P., Chin T.L., Silliman C.C., et al. Hyperfibrinolysis, physiologic fibrinolysis, and fibrinolysis shutdown: the spectrum of postinjury fibrinolysis and relevance to antifibrinolytic therapy. J Trauma Acute Care Surg. 2014;77:811–817. discussion 817. - PMC - PubMed
-
- Branco B.C., Inaba K., Ives C., Okoye O., Shulman I., David J.S., et al. Thromboelastogram evaluation of the impact of hypercoagulability in trauma patients. Shock. 2014;41:200–207. - PubMed
LinkOut - more resources
Full Text Sources
