

Prospective randomized evaluation of the sustained impact of assistive artificial intelligence on anesthetists' ultrasound scanning for regional anesthesia
- PMID: 39430867
- PMCID: PMC11487881
- DOI: 10.1136/bmjsit-2024-000264
Prospective randomized evaluation of the sustained impact of assistive artificial intelligence on anesthetists' ultrasound scanning for regional anesthesia
Abstract
Objectives: Ultrasound-guided regional anesthesia (UGRA) relies on acquiring and interpreting an appropriate view of sonoanatomy. Artificial intelligence (AI) has the potential to aid this by applying a color overlay to key sonoanatomical structures.The primary aim was to determine whether an AI-generated color overlay was associated with a difference in participants' ability to identify an appropriate block view over a 2-month period after a standardized teaching session (as judged by a blinded assessor). Secondary outcomes included the ability to identify an appropriate block view (unblinded assessor), global rating score and participant confidence scores.
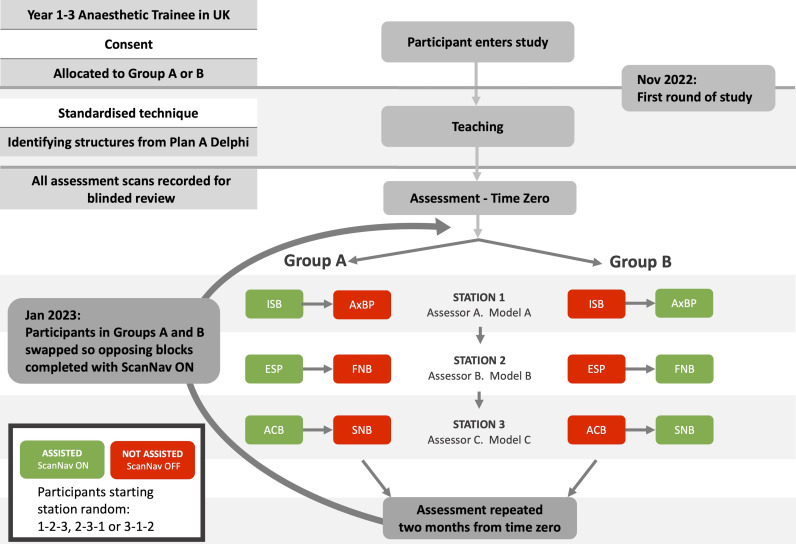
Design: Randomized, partially blinded, prospective cross-over study.
Setting: Simulation scans on healthy volunteers. Initial assessments on 29 November 2022 and 30 November 2022, with follow-up on 25 January 2023 - 27 January 2023.
Participants: 57 junior anesthetists undertook initial assessments and 51 (89.47%) returned at 2 months.
Intervention: Participants performed ultrasound scans for six peripheral nerve blocks, with AI assistance randomized to half of the blocks. Cross-over assignment was employed for 2 months.
Main outcome measures: Blinded experts assessed whether the block view acquired was acceptable (yes/no). Unblinded experts also assessed this parameter and provided a global performance rating (0-100). Participants reported scan confidence (0-100).
Results: AI assistance was associated with a higher rate of appropriate block view acquisition in both blinded and unblinded assessments (p=0.02 and <0.01, respectively). Participant confidence and expert rating scores were superior throughout (all p<0.01).
Conclusions: Assistive AI was associated with superior ultrasound scanning performance 2 months after formal teaching. It may aid application of sonoanatomical knowledge and skills gained in teaching, to support delivery of UGRA beyond the immediate post-teaching period.
Trial registration number: www.clinicaltrials.govNCT05583032.
Keywords: Device Evaluation; Devices; Technology.
Copyright © Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
JSB is a Senior Clinical Advisor for GE Healthcare (and previously Intelligent Ultrasound, receiving research funding and honoraria). MM was employed by Intelligent Ultrasound as a medical writer during this study. DBSL is a clinical advisor for Intelligent Ultrasound, receiving honoraria. NH is the President of Regional Anaesthesia UK. AJRM is the immediate Past-President of Regional Anaesthesia UK and has received honoraria from Intelligent Ultrasound and GE Healthcare. AP is a Past-President of Regional Anaesthesia UK, has received honoraria from GE Healthcare and has consulted for Pacira Biosciences. TA, MPS, AT and JW are board members of Regional Anaesthesia UK. JAN is a senior scientific advisor for Intelligent Ultrasound.
Figures
References
-
- Sites BD, Chan VW, Neal JM, et al. The American Society of Regional Anesthesia and Pain Medicine and the European Society Of Regional Anaesthesia and Pain Therapy Joint Committee recommendations for education and training in ultrasound-guided regional anesthesia. Reg Anesth Pain Med. 2009;34:40–6. doi: 10.1097/AAP.0b013e3181926779. - DOI - PubMed
-
- Henderson M, Dolan J. Challenges, solutions, and advances in ultrasound-guided regional anaesthesia. BJA Educ. 2016;16:374–80. doi: 10.1093/bjaed/mkw026. - DOI
Associated data
LinkOut - more resources
Full Text Sources
Medical