

Colchicine for secondary prevention of ischaemic stroke and atherosclerotic events: a meta-analysis of randomised trials
- PMID: 39431112
- PMCID: PMC11490869
- DOI: 10.1016/j.eclinm.2024.102835
Colchicine for secondary prevention of ischaemic stroke and atherosclerotic events: a meta-analysis of randomised trials
Abstract
Background: Guidelines recommend low-dose colchicine for secondary prevention in cardiovascular disease, but uncertainty remains concerning its efficacy for stroke, efficacy in key subgroups and about uncommon but serious safety outcomes.
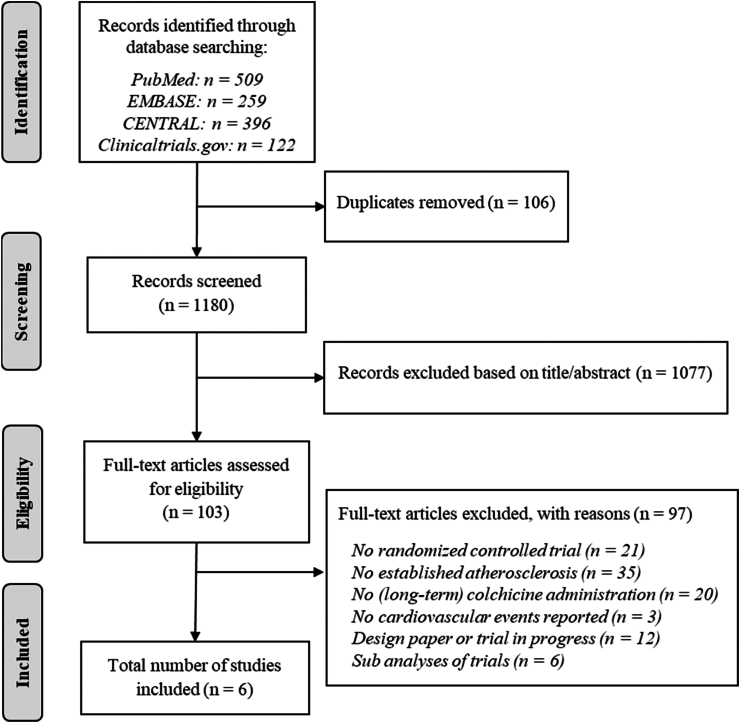
Methods: In this trial-level meta-analysis, we searched bibliographic databases and trial registries form inception to May 16, 2024. We included randomised trials of colchicine for secondary prevention of ischaemic stroke and major adverse cardiovascular events (MACE: ischaemic stroke, myocardial infarction, coronary revascularisation, or cardiovascular death). Secondary outcomes were serious safety outcomes and mortality. A fixed-effect inverse-variance model was used to generate a pooled estimate of relative risk (RR) with 95% confidence intervals (CI). This study is registered with PROSPERO, CRD42024540320.
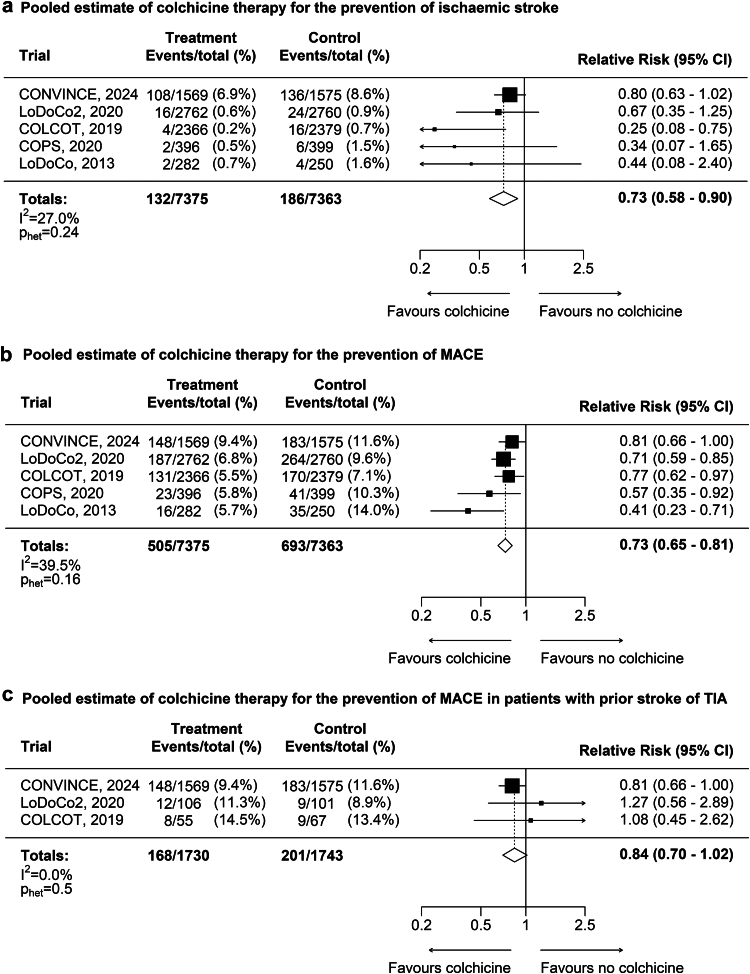
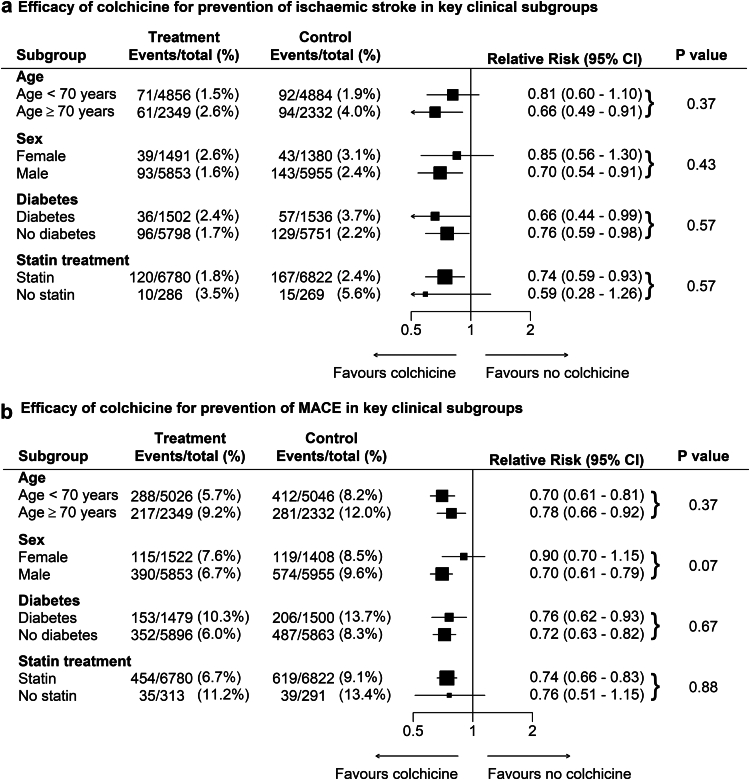
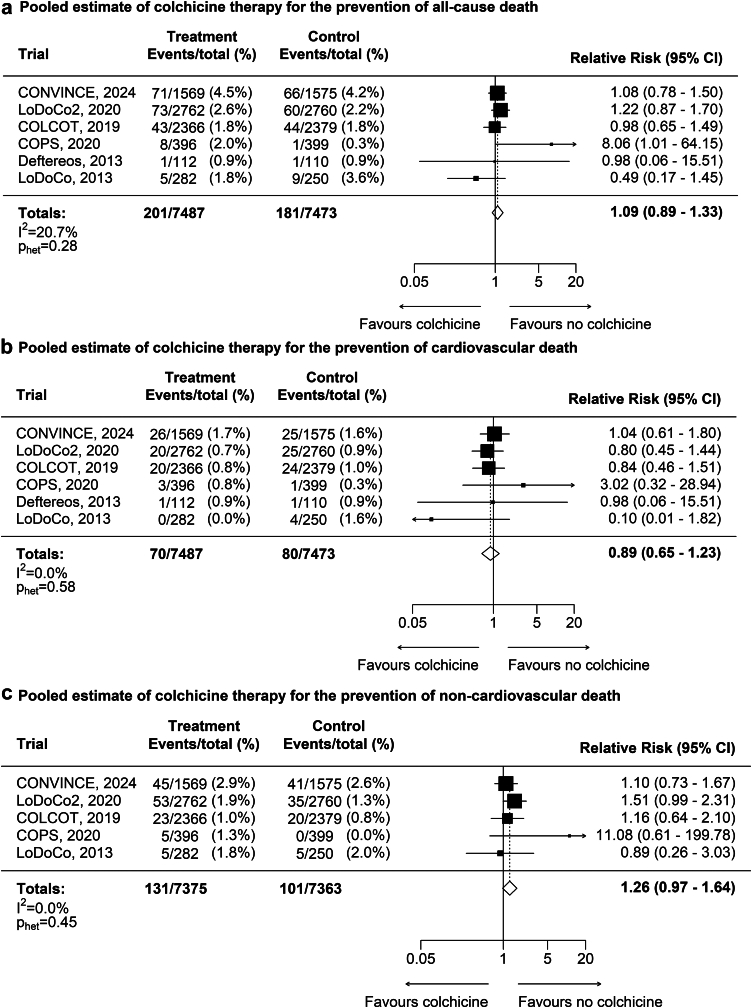
Findings: Six trials involving 14,934 patients with prior stroke or coronary disease were included. In all patients, colchicine compared with placebo or no colchicine reduced the risk for ischaemic stroke by 27% (132 [1.8%] events versus 186 [2.5%] events, RR 0.73 [95% CI 0.58-0.90]) and MACE by 27% (505 [6.8%] events versus 693 [9.4%] events, with RR 0.73 [0.65-0.81]). Efficacy was consistent in key subgroups (females versus males, age below versus above 70, with versus without diabetes, statin versus non-statin users). Colchicine was not associated with an increase in serious safety outcomes: hospitalisation for pneumonia (109 [1.5%] versus 106 [1.5%], RR 0.99 [0.76-1.30]), cancer (247 [3.5%] versus 255 [3.6%], RR 0.97 [0.82-1.15]), and gastro-intestinal events (153 [2.1%] versus 135 [1.9%]), RR 1.15 [0.91-1.44]. There was no difference in all-cause death (201 [2.7%] versus 181 [2.4%], RR 1.09 [0.89-1.33]), cardiovascular death (70 [0.9%] versus 80 [1.1%], RR 0.89 [0.65-1.23]), or non-cardiovascular death (131 [1.8%] versus 101 [1.4%], RR 1.26 [0.98-1.64]).
Interpretation: In patients with prior stroke or coronary disease, colchicine reduced ischaemic stroke and MACE, with consistent treatment effect in key subgroups, and did not increase serious safety events or death.
Funding: There was no funding source for this study.
Keywords: Colchicine; MACE; Meta-analysis; Safety; Stroke.
© 2024 The Authors.
Conflict of interest statement
Funding: Michiel Poorthuis reports support for travel to Dublin from Dr. Jan Meerwaldt stichting. Pierre Amarenco reports grants from the French Government for Reducing Inflammation in Ischemic Stroke with Colchicine (RIISC); Ticagrelor in High-risk patients-Extended Treatment in Ischemic Stroke (THETIS); Treat Stroke to Target 40; Treat Stroke to Target Cholesterol and Colchicine in Cerebral Small Vessel Disease (TST 3C SVD), from Pfizer for Treat Stroke to Target Trial, consulties fees from Neuraltide for TIDE-IN Trial, honoraria from Novartis, Sanofi, and Viatris, support from Novartis, Participation on a Data Safety Monitoring Board or Advisory Board for Cell Prothera, and from AstraZeneca for Ticagrelor supply (Ticagrelor in High-risk patients-Extended Treatment in Ischemic Stroke (THETIS)). Kevin Boczar reports grants from Novartis paid to his institution. Noel Chan is supported by a Heart and Stroke of Canada New Investigator Award, and received a project grant from the Canadian Institutes of Health Research for a randomized trial investigating the risk-benefit of colchicine in peripheral artery disease. Sanjit Jolly reports honoraria from Pharmascience. Binita Shah reports grants from NIH NHLBI and VA Office of Research and Development paid to her institution, support for attending meetings and/or travel from NovoNordisk as US national leader and co-chair of the global expert panel for the ARTEMIS trial, leadership or fiduciary role for the Society of Cardiovascular Angiography and Interventions (Board of Trustees) and the American Heart Association (Associate Editor for Circulation Cardiovascular Intervention), and from Philips Volcano (advisory board). Jean-Claude Tardif reports grants from Amarin, AstraZeneca, Ceapro, DalCor Pharmaceuticals, Esperion, Ionis, Merck, Novartis, Pfizer paid tot his institution, consulting fees from DalCor Pharmaceuticals paid to him, honoraria for lectures from HLS Pharmaceuticals, Pendopharm, Pfizer paid to him, patent for Pharmacogenomics-guided CETP inhibition (waived his right in this patent), patent for Use of colchicine after myocardial infarction (his institution submitted a patent on this topic and he was an author, but waived his rights in this patent and did not stand to gain financially), and a minor equity interest in DalCor Pharmaceuticals. John Eikelboom reports grants from Anthos, Bayer, BI, BMS, Daiichi-Sankyo, Ionis, Janssen, Merck, Pfizer, USV; consulting fees from Anthos, Bayer, BI, BMS, Daiichi-Sankyo, Ionis, Janssen, Merck, Pfizer, USV.
Figures
References
-
- Roth G.A., Huffman M.D., Moran A.E., et al. Global and regional patterns in cardiovascular mortality from 1990 to 2013. Circulation. 2015;132:1667–1678. - PubMed
-
- Kuo H.-K., Yen C.-J., Chang C.-H., Kuo C.-K., Chen J.-H., Sorond F. Relation of C-reactive protein to stroke, cognitive disorders, and depression in the general population: systematic review and meta-analysis. Lancet Neurol. 2005;4:371–380. - PubMed
LinkOut - more resources
Full Text Sources
