

Diagnostic Utility of SARS-CoV-2 Nucleocapsid Antigenemia: A Meta-analysis
- PMID: 39431150
- PMCID: PMC11487748
- DOI: 10.1093/ofid/ofae561
Diagnostic Utility of SARS-CoV-2 Nucleocapsid Antigenemia: A Meta-analysis
Abstract
Background: Studies of the diagnostic performance of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) nucleocapsid antigen in blood (antigenemia) have reached variable conclusions. The potential utility of antigenemia measurements as a clinical diagnostic test needs clarification.
Methods: We performed a systematic review of Pubmed, Embase, and Scopus through July 15, 2023, and requested source data from corresponding authors.
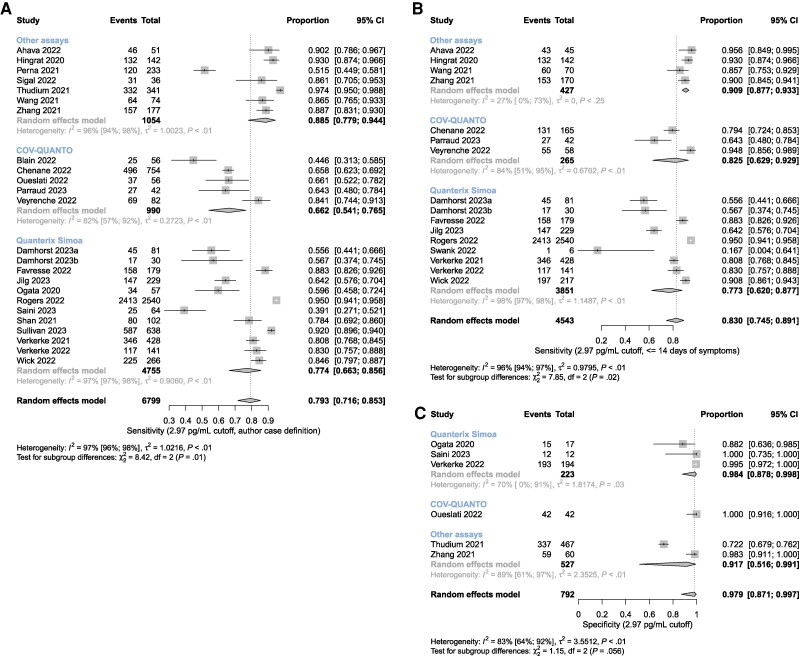
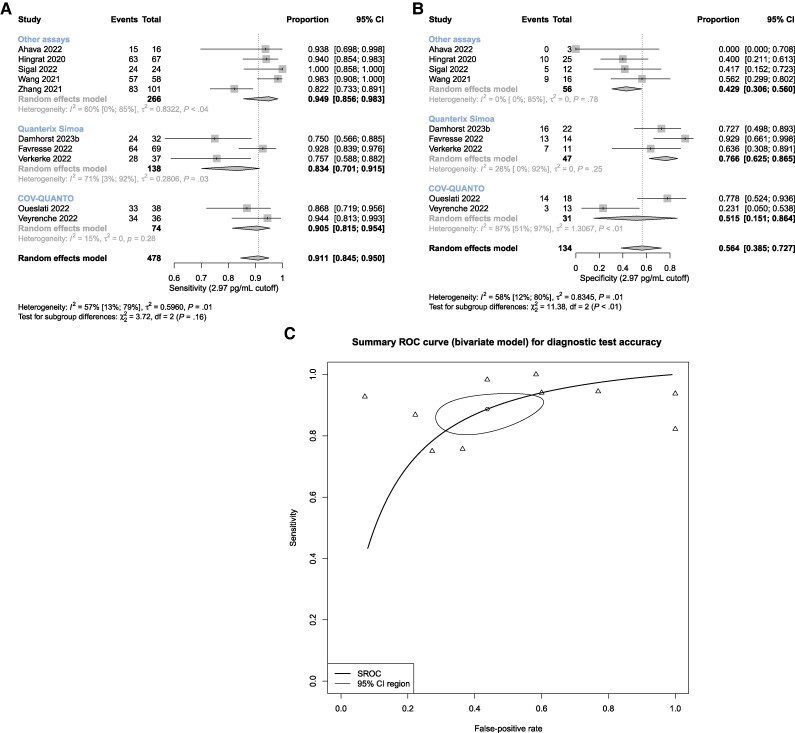
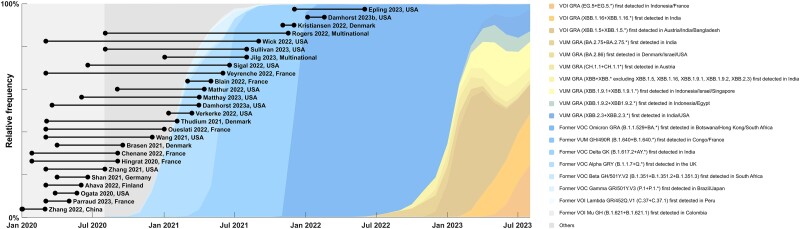
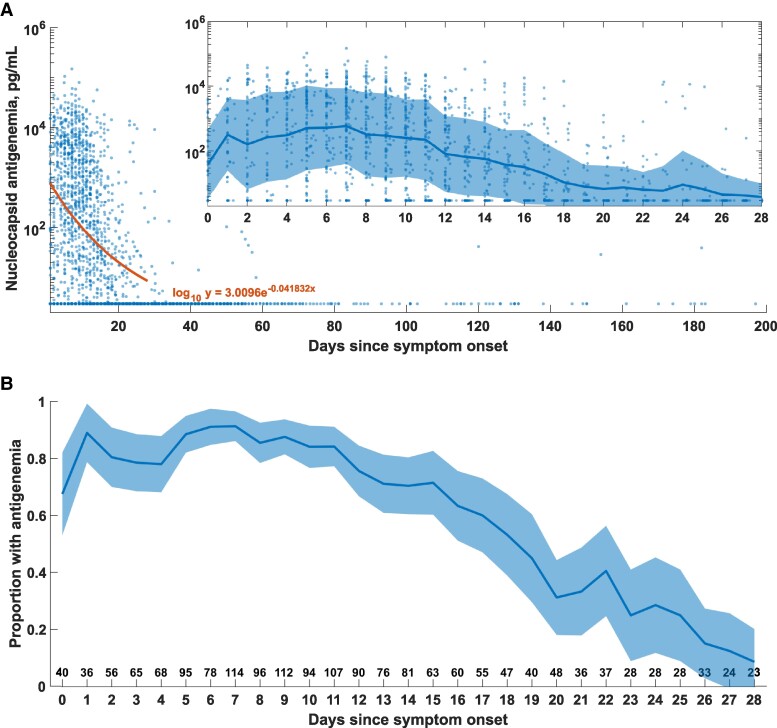
Results: Summary sensitivity from 16 studies (4543 cases) sampled at ≤14 days of symptoms was 0.83 (0.75-0.89), and specificity was 0.98 (0.87-1.00) from 6 studies (792 reverse transcription polymerase chain reaction-negative controls). Summary sensitivity and specificity for paired respiratory specimens with cycle threshold values ≤33 were 0.91 (0.85-0.95) and 0.56 (0.39-0.73) from 10 studies (612 individuals). Source data from 1779 cases reveal that >70% have antigenemia 2 weeks following symptom onset, which persists in <10% at 28 days. The available studies suffer from heterogeneity, and Omicron-era data are scarce.
Conclusions: Nucleocapsid antigenemia currently has limited utility due to limitations of existing studies and lack of Omicron-era data. Improved study designs targeting potential clinical uses in screening, surveillance, and complex clinical decision-making-especially in immunocompromised patients-are needed.
Keywords: SARS-CoV-2; antigenemia; nucleocapsid.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. The authors have no conflicts of interest to disclose.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
